MedicalResearch.com Interview with:
Anna Roca PhD
MRC Unit The Gambia at the London School of Hygiene and Tropical Medicine
Fajara, The Gambia
MedicalResearch.com: What is the background for this study?Response: Context specific interventions are needed to decrease the high burden of severe neonatal morbidity and mortality in sub-Saharan Africa. Severe bacterial infections are a main cause of neonatal mortality in the continent. Oral intra-partum azithromycin is a cheap intervention easily scalable. Before embarking on this trial, we conducted a proof-of-concept trial that showed the intervention reduced maternal and neonatal bacterial carriage of the most prevalent bacteria causing neonatal sepsis in the continent.
(more…)
William A. Petri, MD PhD
Wade Hampton Frost Professor of Medicine and
Vice Chair for Research of the Department of Medicine
Professor of Medicine, Microbiology, Immunology and Cancer Biology, and Pathology,
Medicine: Infectious Diseases and International Health,
Medicine: Infectious Diseases and International Health
MedicalResearch.com: What is the background for this study?MedicalResearch.com We tested if prophylactic antibiotics could prevent sepsis and death in women in the late stages of normal vaginal labor and delivery. It was previously known that antibiotic were effective for this purpose in women undergoing C-section. The study was a randomized placebo-controlled trial at 8 international sites of nearly 30,000 women.
(more…)
MedicalResearch.com Interview with:
Michael J. Mahan Ph.D.
Professor
Dept of Molecular, Cellular, and Developmental Biology
University of California
Santa Barbara, CA
MedicalResearch.com: What is the background for this study? What are the main findings?Response: Sepsis is the number one cause of death in US hospitals- but few molecular diagnostics and therapies exist for this condition. In the clinic, sepsis is diagnosed by a symptom-based approach that may include kidney or liver failure, blood clotting or bleeding — which is often well after permanent organ damage.
Thus, molecular diagnostics that detect infection at early stages of disease to minimize host injury are sorely needed. (more…)
MedicalResearch.com Interview with:
Chanu Rhee, MD, MPH
Harvard Medical School and Harvard Pilgrim Health Institute
Boston, MA
MedicalResearch.com: What is the background for this study? Response: Sepsis is a leading cause of death, disability, and healthcare costs. This has triggered regulators and hospitals to invest heavily in improving sepsis recognition and care. Most notably, the Centers for Medicare & Medicaid Services (CMS) implemented the Severe Sepsis/Septic Shock Early Management Bundle (SEP-1) by the in October 2015. SEP-1 requires hospitals to report compliance with a 3 and 6 hour sepsis care bundle, which includes initial and repeat lactate measurements, blood culture orders, broad-spectrum antibiotic, specific quantities of fluid boluses for hypotension, vasopressors for persistent hypotension, and documentation of a repeat volume and perfusion assessment for patients with septic shock.
While SEP-1 has helped raise awareness of sepsis and catalyzed sepsis quality improvement initiatives around the country, concerns have been raised about its potential unintended consequences -- particularly around increasing unnecessary broad spectrum antibiotic use -- and the strength of evidence supporting the measure. In this study, we used detailed clinical data from a diverse cohort of hospitals to assess whether SEP-1 implementation was associated with changes in key processes of care and mortality in patients with suspected sepsis.(more…)
MedicalResearch.com Interview with:
Dr. Asim Ahmed MD
co-author of the study
Senior medical director at Karius
MedicalResearch.com: What is the background for this study? Would you briefly explain the basis of the Karius Test?Response: The Karius Test is a non-invasive blood test that uses next-generation sequencing of microbial cell-free DNA to rapidly detect over 1,400 bacteria, DNA viruses, fungi, and other pathogens. Doctors primarily use the test to detect specific causative pathogens, complicated pneumonia, cardiovascular infections, and infections in immunocompromised hosts.
The Karius Test is transforming how doctors diagnose infectious diseases by helping doctors identify the precise pathogens infecting patients.
The Karius Test offers a higher diagnostic yield and faster time-to-diagnosis than conventional tests - with the potential to eliminate invasive diagnostic procedures like biopsies.
(more…)
MedicalResearch.com Interview with:
QiPing Feng, PhD
Division of Clinical Pharmacology
Department of Medicine
Vanderbilt University Medical Center
Nashville, Tennessee
MedicalResearch.com: What is the background for this study?
Response: Sepsis is one of the leading causes of hospital mortality. Yet, there are no specific effective treatments for it. Recent information suggests that drugs that inhibit proprotein convertase subtilisin kexin type 9 (PCSK9) could have potential as a new treatment for sepsis.
We used a genetic approach to test if variation in PCSK9 affected the risk of sepsis.
In patients admitted to hospital with infection, neither variants in the PCSK9 gene nor predicted expression of PCSK9 were associated with risk of sepsis or poorer outcomes after sepsis.(more…)
MedicalResearch.com Interview with:
Minh-Hong Nguyen, MD
Infectious Diseases
Professor of Medicine
Director, Transplant Infectious Diseases
Director, Antimicrobial Management Program
Department of Medicine
University of Pittsburgh School of Medicine
MedicalResearch.com: What is the background for this study? What are the main findings?Response: Blood cultures, the gold standard for diagnosing blood stream infections, are insensitive and limited by prolonged time to results. Early institution of appropriate antibiotics is a crucial determinant of improved outcomes in patients with sepsis and blood stream infections (BSI). For these reasons, development of rapid non-culture diagnostic tests for blood stream infections is a top priority.
The T2Bacteria panel is the first direct from blood, non-culture test cleared by FDA for diagnosis of blood stream infections . It detects within 4-6 hours the 5 most common ESKAPE bacteria that are frequent causes of hospital infection, and which are often multi-drug resistant. This study shows that the T2Bacteria panel rapidly and accurately diagnosed and identified ESKAPE bacterial BSIs, and identified probable and possible BSIs that were missed by blood cultures (in particular among patients who were already receiving antibiotics).
(more…)
MedicalResearch.com Interview with:
Chanu Rhee, MD,MPH
Assistant Professor of Population Medicine
Harvard Medical School / Harvard Pilgrim Health Care Institute
Assistant Hospital Epidemiologist
Brigham and Women’s HospitalMedicalResearch.com: What is the background for this study? Response: Sepsis is the body’s reaction to a serious infection that results a cascade of inflammation in the body and organ dysfunction, such as low blood pressure, confusion, or failure of the lungs, kidneys, or liver. Sepsis is a major cause of death, disability, and cost in the U.S. and around the world. Growing recognition of this problem has led to numerous sepsis performance improvement initiatives in hospitals around the country. Some of these efforts have also been catalyzed by high-profile tragic cases of missed sepsis leading to death, which may have contributed to a perception that most sepsis deaths are preventable if doctors and hospitals were only better at recognizing it.
However, the extent to which sepsis-related deaths might be preventable with better hospital-based care is unknown. In my own experience as a critical care physician, a lot of sepsis patients we treat are extremely sick and even when they receive timely and optimal medical care, many do not survive. This led myself and my colleagues to conduct this study to better understand what types of patients are dying from sepsis and how preventable these deaths might be.(more…)
MedicalResearch.com Interview with:
Dr. Jianguo Xu, MD
West China Hospital, Sichuan University
Chengdu, Sichuan, China
MedicalResearch.com: What is the background for this study? Response: Since the mid-20th century, corticosteroids have been used as adjuvant therapy in the context of sepsis. Although evaluated in numerous randomized clinical trials and meta-analyses, both the safety and efficacy of corticosteroids remain controversial.
(more…)
MedicalResearch.com Interview with: Daniel J. Lane PhD Institute of Health Policy, Management and Evaluation Dalla Lana School of Public Health, University of Toronto Rescu, Li Ka Shing Knowledge Institute, St Michael’s Hospital Toronto, Ontario, Canada
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Early resuscitation and early antibiotics have become the mainstay treatment for patients with sepsis. The time to initiation of these treatments is thought to be an important factor in patients surviving their disease; however, the independent benefits or harms of intravenous fluid resuscitation, in particular a more aggressive versus more conservative approach to this therapy, remains difficult to evaluate given the concurrent use of these therapies in hospital.
To gain a better understanding of this treatment independent of antibiotic use, we assessed intravenous fluid resuscitation by paramedics on the in-hospital mortality of patients with sepsis. By accounting for the interaction between initial systolic blood pressure and the treatment, we found that earlier resuscitation by paramedics was associated with decreased mortality in patients with low initial blood pressures but not associated with mortality for patients with normal or higher initial blood pressures.
MedicalResearch.com Interview with:
Idris V.R. Evans, M.D.,MA
Assistant Professor
Department of Critical Care Medicine
University of Pittsburgh
MedicalResearch.com: What is the background for this study? What are the main findings?Response: New York State issued a state-wide mandate in 2013 for all hospitals to develop protocols for sepsis recognition and treatment. This mandate was called “Rory’s Regulations” in honor of Rory Staunton, a boy who died from sepsis in 2012.
Pediatric protocols involved a bundle of care that included blood cultures, antibiotics, and an intravenous fluid bolus within 1–hour. We analyzed data collected by the NYS Department of Health on 1,179 patients from 54 hospitals and found that the completion of the pediatric bundle within 1 hour was associated with a 40% decrease in the odds of mortality.(more…)
MedicalResearch.com Interview with:
Becky Jayakumar, PharmDCollege of PharmacyAssistant Professor of Pharmacy Practice
Roseman University of Health Sciences
MedicalResearch.com: What is the background for this study? What are the main findings?Response: Bacteremia (bloodstream infections) due to Gram-negative (GN) bacteria are a frequent cause of severe sepsis and pose serious therapeutic challenges due to multidrug-resistance (MDR). Ceftolozane/tazobactam (C/T) is a novel antipseudomonal cephalosporin combined with an established β-lactamase inhibitor.
This retrospective, observational study evaluated the clinical outcomes of C/T real-world use in severely ill patients. Twenty-two patients with sepsis and/or bacteremia were included; 95% of whom had Pseudomonas aeruginosa that was resistant to almost all antibacterials with the exception of colistin. C/T successfully treated the majority of these complicated patients. In this real-world study, 77% of patients had a clinical response with C/T and 75% had a microbiological response. Clinical success rates were high and mortality rates were similar to other studies in this severely ill population. (more…)
MedicalResearch.com Interview with:
Amanda Paschke, MD, MSCE
Senior principal scientist
Infectious disease clinical research
Merck Research Laboratories
MedicalResearch.com: What is the background for this study? What are the main findings?Response: This study sought to evaluate a new beta-lactam/beta-lactamase inhibitor antibacterial combination, imipenem/relebactam (IMI/REL), compared with colistin plus imipenem for the treatment of infections caused by resistant Gram-negative bacteria.
Patients enrolled in the trial had hospital-acquired or ventilator-associated bacterial pneumonia (HABP/VABP), complicated intra-abdominal infections (cIAI), or complicated urinary tract infections (cUTI) caused by pathogens that were non susceptible to imipenem, a carbapenem antibacterial.
In this study, the primary outcome was a favorable overall response to treatment, which was comparable between the IMI/REL vs colistin + IMI arms. Colistin (often combined with a carbapenem) is currently among the standard of care treatment regimens for MDR infections. A key secondary endpoint of the study was safety. IMI/REL was well tolerated; among all treated patients, drug-related adverse events (AEs) occurred in 16.1% of IMI/REL and 31.3% of colistin + IMI patients with treatment-emergent nephrotoxicity observed in 10% (3/29 patients) and 56% (9/16 patients), respectively (p=0.002). Results of the trial support the use of imipenem-relebactam (IMI/REL) as an efficacious and well-tolerated treatment option for carbapenem-resistant infections.(more…)
MedicalResearch.com Interview with:
Bala Venkatesh, MBBS, MD(Int.Med), FRCA, FFARCSI, MD(UK), FCICM
Director of Intensive Care, Wesley Hospital
Pre-eminent specialist, Princess Alexandra Hospital
Professor of Intensive Care,University of QLD
Honorary Professor, University of New South WalesProfessorial Fellow, The George Institute for Global Health
MedicalResearch.com: What is the background for this study? What are the main findings?Response: Whether hydrocortisone reduces mortality in patients with septic shock is unclear. The uncertainty about the efficacy of glucocorticoids in reducing mortality in patients with septic shock has resulted in widespread variation in clinical practice
In the results published in the New England Journal of Medicine the investigators found steroids not only reduced the duration of septic shock, they also led to less blood transfusions, and the time spent on life support therapy in intensive care. However, the use of steroids did not lead to fewer deaths overall compared to placebo.
Some of the findings are consistent with previous research whilst other results add new information that will inform clinicians.
Our results show there is still a lot to learn about septic shock which kills up to half of those affected in some parts of the world. There are undoubtedly many other contributors to survival which we don’t yet understand.(more…)
MedicalResearch.com Interview with:
Dr. Robert Hiensch MD
Assistant Professor, Medicine, Pulmonary, Critical Care and Sleep Medicine
Icahn School of Medicine at Mount Sinai.
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: New sepsis guidelines that recommend screening and early treatment for sepsis cases appear to have significant positive impacts on patient outcomes. Less research has been published on what potential side effects may result from these guidelines.
Antibiotics are a cornerstone of sepsis treatment and early antibiotic administration is strongly recommended. We examined whether the introduction of an electronic based sepsis initiative changed antibiotic prescribing patterns at our hospital. Antibiotics, even when appropriate, contribute to hospital onset Clostridium difficile infections (HO CDIs). While the authors do not dispute the importance of antibiotic administration in sepsis, it is valuable to know whether the sepsis initiative coincided with both increased antibiotic administration and HO CDIs.
(more…)
MedicalResearch.com Interview with:
Dr. Chanu Rhee MD, Assistant Professor
Therapeutics Research and Infectious Disease Epidemiology Group
Department of Population Medicine at Harvard Medical School / Harvard Pilgrim Health Care Institute
Critical Care and Infectious Disease Physician
Transplant/Oncology Infectious Disease service and
Medical Intensive Care Unit at Brigham and Women’s Hospital
MedicalResearch.com: What is the background for this study?
Response: Multiple studies suggest that the incidence of sepsis, the syndrome of life-threatening organ dysfunction caused by infection, is increasing over time, while mortality rates are decreasing. However, reliably measuring sepsis incidence and trends is challenging because clinical diagnoses of sepsis are subjective and insurance claims data, the traditional method of surveillance, can be affected by changing diagnosis and coding practices over time.
In this study, my colleagues and I estimated the current U.S. burden of sepsis and trends using clinical data from the electronic health record systems of a large number of diverse hospitals. The findings, published in JAMA, challenge the use of claims data for sepsis surveillance and suggest that clinical surveillance using electronic health record data provides more objective estimates of sepsis incidence and outcomes.
(more…)
MedicalResearch.com Interview with:
Christopher W. Seymour, M.D., M.Sc.
Assistant professor of Critical Care Medicine and Emergency Medicine, and member of Clinical Research Investigation and Systems Modeling of Acute Illness
University of Pittsburgh
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Following the tragic and widely publicized death of Rory Staunton, 12, from undiagnosed sepsis in 2012, New York became the first state to require that hospitals follow a protocol to quickly identify and treat the condition. The mandate led to widespread controversy in the medical community as to whether such steps would have saved Rory or anyone else’s life.
Rory’s Regulations require hospitals to follow protocols for early identification and treatment of sepsis, and submit data on compliance and outcomes. The hospitals can tailor how they implement the protocols, but must include a blood culture to test for infection, measurement of blood lactate (a sign of tissue stress) and administration of antibiotics within three hours of diagnosis—collectively known as the “three-hour bundle.”
We analyzed data from nearly 50,000 patients from 149 New York hospitals to scientifically determine if Rory’s Regulations worked. We found that they did - 83 percent of the hospitals completed the bundle within the required three hours, overall averaging 1.3 hours for completion. For every hour that it took clinicians to complete the bundle, the odds of the patient dying increased by 4 percent.
(more…)
MedicalResearch.com Interview with:
Faheem Guirgis MD
Assistant Professor of Emergency Medicine
Department of Emergency Medicine
Division of Research
UF Health Jacksonville
MedicalResearch.com: What is the background for this study? What are the main findings?Response: Sepsis is quite prevalent among hospitals and the incidence is increasing. It is a life-threatening disease that can lead to poor outcomes if patients are not recognized and treated promptly. We recognized that our institution needed a strategic approach to the problem of sepsis, therefore the Sepsis Committee was created with the goal of creating a comprehensive sepsis program.
We developed a system for sepsis recognition and rapid care delivery that would work in any area of the hospital. We found that we reduced overall mortality from sepsis, the number of patients requiring mechanical ventilation, intensive care unit length and overall hospital length of stay, and the charges to the patient by approximately $7000 per patient.
(more…)
MedicalResearch.com Interview with:
Anish Agarwal, MD, MPH
The Hospital of the University of Pennsylvania
Department of Emergency Medicine
Philadelphia, PA
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: The morbidity and mortality of severe sepsis has been well studied and documented. An aggressive approach to protocolized care for patients suffering from severe sepsis and septic shock has been shown to improve mortality and should be started as early in the time course of a patient's presentation. Emergency departments (ED) are designed to deliver time-sensitive therapies, however, they also may suffer from crowding due to multiple factors.
This study aimed to assess the impact of ED crowding upon critical interventions in the treatment of severe sepsis including time to intravenous fluids, antibiotics, and overall delivery of a protocolized bundle of care. The study found that as ED crowding increased, time to critical therapies significantly increased and the overall implementation of procotolized care decreased. More specifically as ED occupancy and total patient hours within the ED increased, time to intravenous fluids decreased and time to antibiotics increased as occupancy, hours, and boarding increased.
(more…)
MedicalResearch.com Interview with:Sachin Yende, M.D., M.S., Associate professor
University of Pittsburgh School of Medicine’s departments of
Critical Care Medicine and Clinical and Translational and
Vice president of Critical Care at the VA Pittsburgh.
Florian B. Mayr, M.D., M.P.H.
Faculty member in University of Pittsburgh
Department of Critical Care Medicine and the
Center for Health Equity Research and Promotion
MedicalResearch.com: What is the background for this study? What are the main findings?Response: The Centers for Medicare and Medicaid Services and the Veteran Health Administration currently track readmission rates for pneumonia, acute heart attacks, heart failure and chronic obstructive lung disease for quality purposes and pay for performance. In our study, we were able to demonstrate that unplanned readmissions after sepsis (defined as life threatening organ failure due to the body's response to an overwhelming infection) are more common than readmission for these other conditions stated above and associated with significant excess costs.
(more…)
MedicalResearch.com Interview with:
Halden F. Scott MD, Assistant Professor
Departments of Pediatrics and Emergency Medicine
University of Colorado School of Medicine
MedicalResearch.com: What is the background for this study?Response: Sepsis, a dysregulated immune response to infection, is a leading cause of death for children. Survival depends on rapid diagnosis and timely delivery of life-saving resuscitative care, including fluids and antibiotics. However, it can be challenging to make an early diagnosis of sepsis in children.
Millions of children present for emergency care of infection and fever every year, most of whom will not develop sepsis. Tools that assist providers in distinguishing the sickest children with infection at an early stage could enable the early delivery of life-saving treatments.
Lactate is a clinically-available laboratory test that has played a critical role in improving the diagnosis and treatment of sepsis in adults. Sepsis may cause lactate levels to rise in the blood during sepsis, through reduced delivery of oxygen to the tissues, as well as through changes in how energy is produced and in how lactate is cleared by the kidney and liver. Data about lactate in pediatric sepsis, particularly early levels and whether it is associated with mortality, have been limited.
(more…)
MedicalResearch.com Interview with:Jochen Gensichen, MD, MSc, MPH
Institute of General Practice and Family Medicine
Konrad Reinhart, MD
Center of Sepsis Control and Care
Jena University Hospital
Friedrich-Schiller-University
School of Medicine
Jena, GermanyMedicalResearch.com: What are the main findings?Response: Sepsis survivors face multiple long-term sequelae which result in increased primary care needs as a basic support in medication, physiotherapy or mental health. Process of care after discharge from the intensive care unit often is fragmented.
(more…)
MedicalResearch.com Interview with:
Leo McHugh, Ph.D.
Director, Bioinformatics
Immunexpress
Seattle, WashingtonMedical Research: What is the background for this study? What are the main findings?
Dr. McHugh: Sepsis is the leading cause of child mortality in the world, and in developing countries kills more adults than breast cancer, prostate cancer and HIV combined. Approximately 30% of people admitted to ICU have sepsis, and up to 50% of these patients die. It’s a major cost burden also, costing the US health system $17 billion per year. The best way to reduce costs and improve patient outcomes is to detect sepsis early and with confidence, so that appropriate treatments can be applied. Each hour delay in the detection of sepsis has been reported to correspond to an 8% increase in mortality. So the need for a rapid and accurate diagnostic is recognized. Traditional methods rely on detection of the specific pathogen causing the infection, and these methods often take more than 24 hours, and find a pathogen in only 30% of clinically confirmed cases because they’re trying to detect a minuscule amount of pathogen or pathogenic product in the blood. Our approach was to use the host’s own immune system, which is highly tuned to respond to the presence of pathogens. Around 30% of all genes are dysregulated in sepsis, so there is a huge signal base to draw from. The trick with using multi marker host response is to pick out the specific combination of gene expression patterns that cover the broad range of patients that present with sepsis and who may present either early or late in the episode, thus with different gene activation patterns.
This paper describes a simple combination of such genes that can be used to detect sepsis and performs over the full range of patients irrespective of stage of infection or severity of infection. In it’s current format, the test is manual and takes 4-6 hours, and is a great advance on the current tools, however the methods we’ve used are specifically designed to meet requirements to port this assay onto a fully automated Point of Care platform that could deliver a result in under 90 minutes.
(more…)
MedicalResearch.com Interview with:
Dr. Pablo Moreno Franco MD
Assistant Professor of Medicine
MAYO Clinic
Medical Research: What is the background for this study? What are the main findings?
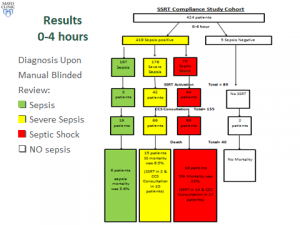
Dr. Pablo Franco: Early alerts and prompt management of patient with severe sepsis and septic shock (SS/S) starting in the emergency department (ED) have been shown to improve mortality and other pertinent outcomes. With this in mind, we formed a multidisciplinary sepsis and shock response team (SSRT) in September 2013. Automated electronic sniffer alerted ED providers for possible sepsis and when S/SS was identified, they were encouraged to activate SSRT.
Two blinded reviewers retrospectively abstracted data on clinical trajectory and outcomes of all patients with sepsis and SS/S admitted at a single academic medical center between September 2013 and September 2014. Given importance of timely recognition and interventions in S/SS, we specifically focused on 2 periods: 0-4 hours and 4-12 hours after hospital admission. Additionally, we compared the compliance to “standard of care” between the SSRT pre-implementation period and the study period.
There were 167 patients admitted with sepsis, among which there were 3 SSRT activations and sepsis mortality was 3.6%. There were 176 patients with SS, SSRT was called in 42 (23%) and SS mortality was 8.5%. CCS was involved in 66 patients and mortality was 6.9% if SSRT was activated, versus 21.6% if SSRT was not activated. There were 76 patients with septic shock, SSRT was called in 44 (57%) and septic shock mortality was 25%. Critical Care Service (CCS) was involved in 68 patients and mortality rates with and without SSRT were 30.9% and 15.4%, respectively. The all-or-none compliance with applicable goals of resuscitation improved from the baseline 0% to over 50% at the study period end. Overall observed/expected sepsis mortality index improved from 1.38 pre-SSRT to 0.68 post-SSRT implementation.
(more…)
MedicalResearch.com Interview with:
Hallie Prescott, MD, MSc
Clinical Lecturer, Internal Medicine
Division of Pulmonary & Critical Care Medicine
University of Michigan Health System
Ann Arbor, MI 48109-2800
Medical Research: What is the background for this study? What are the main findings?
Dr. Prescott: The post-hospital period has been widely recognized as a vulnerable time for patients. In particular, patients who survive sepsis are frequently readmitted to the hospital in the following three months.
In this study, we examined data from 2,600 survivors of sepsis, a severe infection that leads to organ failure. About 42% of the sepsis patients were readmitted in the next 90 days, similar to the rate seen for patients hospitalized for other acute conditions.
However, the reasons for hospital readmission after sepsis are different. A greater number of patients are re-hospitalized for “ambulatory-care sensitive conditions”, which are conditions that could potentially be prevented or treated early in the outpatient setting to avoid a hospital stay.
(more…)
MedicalResearch.com Interview with:
Daniel Irimia, M.D., Ph.D.
Assistant Professor
Division of Surgery, Science & Bioengineering
Massachusetts General Hospital and Harvard Medical School
Associate Director, BioMEMS Resource Center
Boston, MA 02129
Medical Research: What is the background for this study? What are the main findings?
Response: Sepsis is affecting more than half of the patients with major burn injuries (20 percent of body surface) and is the leading cause of death among these patients. Sepsis is also a significant complication for other critically ill patients. More than one million Americans are affected and it has been estimated that approximately 30% of these people die, despite significant advances in life support and antibiotics. Early diagnosis is essential, and it has been calculated that every 6 hours of delay in a sepsis diagnosis decreases the chances of survival by 10 percent.
We have found that the motility of the white blood cells called neutrophils, inside a microfluidic device, is significantly altered two to three days before sepsis develops. (more…)
MedicalResearch.com Interview with: Mark E Mikkelsen, MD, MSCE
Assistant Professor of Medicine
Hospital of the University of Pennsylvania
Medical Research: What is the background for this study? What are the main findings?Dr. Mikkelsen: Sepsis is common, afflicting as many as 3 million Americans each year. It is also costly, both in terms of health care expenditures that exceed $20 billion for acute care and in terms of the impact it has on patients and their families. To date, studies have focused on what happens to septic shock patients during the initial hospitalization. However, because more patients are surviving sepsis than ever, we sought to examine the enduring impact of septic shock post-discharge. We focused on the first 30 days after discharge and asked several simple questions. First, how often did patients require re-hospitalization after septic shock? And second, why were patients re-hospitalized?
We found that 23% of septic shock survivors were re-hospitalized within 30 days, many of them within 2 weeks. A life-threatening condition such as recurrent infection was the reason for readmission and 16% of readmissions resulted in death or a transition to hospice.
(more…)
MedicalResearch.com Interview with: Dr R.E.W. (Bob) Hancock, OC, OBC, FRSC
{Canada Research Chair and Professor, Department of Microbiology and Immunology,UBC}
Director, Centre for Microbial Diseases and Immunity Research
University of British Columbia,
Vancouver, British Columbia, Canada
MedicalResearch: What is the background for this study? What are the main findings?Dr. Hancock: We wanted to understand how patients transitioned from the hyperinflammatory phase (cytokine storm) of sepsis to the hypoinflammatory (immunosuppressive) phase of sepsis (inability to respond appropriately to infections). About 15% of patients die in this first phase and 20% in the second phase, making sepsis one of the most deadly syndromes (35% overall mortality, 5 million deaths [8.3% of all deaths] annually worldwide). We hypothesized that immunosuppression was characterized by a state termed endotoxin tolerance a cellular amnesia (termed cellular reprogramming) in which cells fail to respond to microbial cues.
Overall we found that an Endotoxin Tolerance gene signature is significantly associated with the subsequent development of confirmed sepsis and new organ dysfunction in patients who had suspected sepsis. All 620 sepsis patients in retrospective and new analyses presented with an expression profile strongly associated with the endotoxin tolerance signature (p<0.01; AUC 96.1%). This occurred in fact very early in sepsis and in a new clinical study we found that the signature could be detected already in the emergency ward at first clinical presentation and 24-48 hours prior to definitive diagnosis. Importantly, this signature further differentiated between suspected sepsis patients who did, or did not, go on to develop confirmed sepsis, and predicted the development of organ dysfunction.
(more…)
MedicalResearch.com Interview with:Craig A Umscheid, MD, MSCE, FACP
Assistant Professor of Medicine and Epidemiology
Director, Center for Evidence-based Practice
Medical Director, Clinical Decision Support
Chair, Department of Medicine Quality Committee
Senior Associate Director, ECRI-Penn AHRQ Evidence-based Practice Center, University of Pennsylvania Philadelphia, PA 19104
Medical Research: What are the main findings of the study?Dr. Umscheid: We developed an automated early warning and response system for sepsis that has resulted in a marked increase in sepsis identification and care, transfer to the ICU, and an indication of fewer deaths due to sepsis.
Sepsis is a potentially life-threatening complication of an infection; it can severely impair the body’s organs, causing them to fail. There are as many as three million cases of severe sepsis and 750,000 resulting deaths in the United States annually. Early detection and treatment, typically with antibiotics and intravenous fluids, is critical for survival.
The Penn prediction tool, dubbed the “sepsis sniffer,” uses laboratory and vital-sign data (such as body temperature, heart rate, and blood pressure) in the electronic health record of hospital inpatients to identify those at risk for sepsis. When certain data thresholds are detected, the system automatically sends an electronic communication to physicians, nurses, and other members of a rapid response team who quickly perform a bedside evaluation and take action to stabilize or transfer the patient to the intensive care unit if warranted.
We developed the prediction tool using 4,575 patients admitted to the University of Pennsylvania Health System (UPHS) in October 2011. We then validated the tool during a pre-implementation period from June to September 2012, when data on admitted patients was evaluated and alerts triggered in a database, but no notifications were sent to providers on the ground. Outcomes in that control period were then compared to a post-implementation period from June to September 2013. The total number of patients included in the pre and post periods was 31,093.
(more…)
MedicalResearch.com Interview with: Anders Perner, MD, PhD
Overlæge / Senior staff specialist
Professor / Professor in Intensive Care
Dept of Intensive Care
Rigshospitalet Copenhagen Denmark
Medical Research: What are the main findings of the study?Dr. Perner: In the large international randomised trial, we showed similar outcomes in patients with septic shock with anemia transfused at a lower vs. a higher hemoglobin threshold. The lower threshold group received 50 % fewer transfusions and one-third of these patients were never transfused in ICU.
(more…)
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish.AcceptRejectRead More
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are as essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.