
14 Jan Calcium Artery Score Screening: Cost Effectiveness in Patients with Family History of Early Heart Disease
MedicalResearch.com Interview with:
Prasanna Venkataraman MBBS
Thomas H. Marwick MBBS, PhD
Baker Heart and Diabetes Research Institute
Monash University, Melbourne
Melbourne, Australia
MedicalResearch.com: What is the background for this study?
- Coronary artery calcium score (CAC) quantifies coronary calcium as determined by computed tomography and is a good surrogate marker for overall coronary plaque burden. It can help to reclassify patients at intermediate risk – many of whom are actually at low risk and can be reassured. Conversely, the finding of coronary calcium can also motivate patients (and their clinicians) to more aggressively control their cardiovascular risk factors. This is particularly problematic in those with a family history of premature coronary artery disease, where standard risk prediction tools are less accurate. However, CT CAC does not routinely attract third party payer support limiting its access and utilisation.
- We screened 1084 participants who have a family history of premature coronary disease and a 10-year Pooled cohort Equation (PCE) cardiovascular risk >2% with CAC. We then assessed the cost-effectiveness of commencing statins in those with any coronary calcium compared to a strategy of no CAC testing and commencing statins if their PCE risk was ≥7.5% consistent with current guidelines.
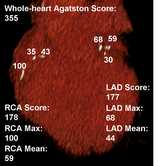
Lesion-specific calcium score. (Wikipedia image)
MedicalResearch.com: What are the main findings?
- A CAC guided strategy increased statin treatment from 27% under standard care to 45% of the CAUGHT-CAD cohort and was highly cost-effective.
- Systematic CT CAC screening was cost-effective and cost-saving for those with baseline 10-year PCE risk 5-7.5% and >7.5% respectively. CAC cost-effectiveness was enhanced if statin treatment was restricted to those with a CAC ≥ 100.
- However, calcium artery score screening was less cost-effective in particular sub-groups including those with baseline PCE<5%, participants aged 40-50 years and female participants.
- Cost-effectiveness was partly driven by avoiding statin treatment in those with zero CACS who would otherwise be recommended therapy.
MedicalResearch.com: What should readers take away from your report?
- Systematic calcium artery score screening in those with a family history of premature coronary artery disease is cost-effective especially when the patient is over the age of 50 or their PCE risk is greater ≥ 5% and the result will impact the decision to commence statins.
- The current approach – using a lower threshold for intervention with standard risk prediction tools in patients with family history of premature CAD – is less likely to be cost-effective.
- Our study supports current efforts to expand access to CAC through third-party reimbursement.
MedicalResearch.com: What recommendations do you have for future research as a result of this work?
- Longer-term, follow-up results from CAUGHT-CAD and other CAC trials are necessary to establish the magnitude of clinical outcome benefits from systematic calcium artery score screening when compared to standard risk assessment.
- Our research highlights the need for more research into non-traditional risk factors to improve risk stratification in otherwise low risk groups in particular those <50 years of age or female.
No disclosures
Citation:
Cost-Effectiveness of Coronary Artery Calcium Scoring in People With a FamilyHistory of Coronary Disease
Prasanna Venkataraman, MB, BS,a,b Hiroshi Kawakami, MD, PHD,a Quan Huynh, PHD,a Geoffrey Mitchell, MBBS, PHD,c Stephen J. Nicholls, MB, BS, PHD,b Tony Stanton, MB, CHB, PHD,c Andrew Tonkin, MD,b Gerald F. Watts, DSC, PHD, MD,d Thomas H. Marwick, MBBS, PHD, MPH,a,b on behalf of the CAUGHT-CAD investigators
JACC: CARDIOVASCULAR IMAGING VOL. -, NO. -, 2021 ª 2021 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION
[wysija_form id=”3″]
[last-modified]
The information on MedicalResearch.com is provided for educational purposes only, and is in no way intended to diagnose, cure, or treat any medical or other condition. Always seek the advice of your physician or other qualified health and ask your doctor any questions you may have regarding a medical condition. In addition to all other limitations and disclaimers in this agreement, service provider and its third party providers disclaim any liability or loss in connection with the content provided on this website.
Last Updated on January 14, 2021 by Marie Benz MD FAAD