
16 Jan The PlaqueTec Liquid Biopsy System™ Allows Detection of Predictive Intracoronary Artery Biomarkers
MedicalResearch.com Interview with:
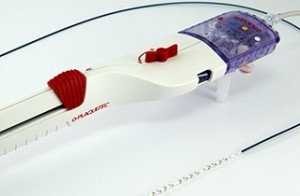
The PlaqueTec Liquid Biopsy System™ (LBS)
Nick West MA MD FRCP FESC FACC
Chief Medical Officer
PlaqueTec Ltd
MedicalResearch.com: What is the background for the Liquid Biopsy System and this study?
Response: Despite huge advances in the diagnosis and treatment of coronary artery disease, this form of cardiovascular disease remains as the world’s number one cause of death. Although interventions such as coronary angioplasty and cholesterol lowering with statins have improved morbidity, patients still experience high rates of recurrent cardiovascular events. Various technologies have been applied to predict future patient events with limited success, such as ‘virtual histology’ intravascular ultrasound (VH-IVUS) in the PROSPECT study (Stone GW et al. N Engl J Med 2011; 364: 226-235). Many experts acknowledge that imaging alone may be insufficient to gauge risk, and that the utility of a more biological endpoint may be more appropriate. This supposition is supported by recent data that added endothelial shear stress estimation to the PROSPECT data and significantly improved subsequent event prediction (Stone PH et al. JACC Cardiovascular Imaging 2017; Sep 18 epub ahead of print).
Coronary artery disease has long been recognised to be underpinned by an inflammatory pathogenesis, and it is bioactive molecules (growth factors, cytokines etc) within the vasculature that affect plaque growth, transformation and vulnerability to rupture, resulting in myocardial infarction. Measuring these biomolecules in situ is challenging owing to an inability to reliably sample from the ‘boundary layer’ – a slower-moving circumferential stratum of blood adjacent to the endothelial surface that does not mix with the general bulk flow.
The PlaqueTec Liquid Biopsy System™ (LBS) was designed specifically to sample from the boundary layer at four sites simultaneously within the coronary artery, where biomolecules released from plaques are likely to be most concentrated. With the LBS, we can also detect small gradients of released molecules by simultaneously collecting blood both upstream and downstream of individual plaques.
The LBS has demonstrated safety and feasibility in preclinical and preliminary clinical studies, and was awarded a CE mark in Europe as a dedicated coronary blood sampling device in 2014.
MedicalResearch.com: What are the main findings?
Response: We analysed data from the first-in-human safety and feasibility study (n = 10) and the first human proof-of-concept evaluation (n = 28) of the PlaqueTec LBS™. The LBS was used in these studies as an adjunct to coronary angioplasty and stent deployment in patients with stable angina pectoris or stabilized non-ST-segment elevation acute coronary syndromes (ACS).
Deployment of theThe PlaqueTec Liquid Biopsy System™ into normal coronary arteries and its use in taking four simultaneous blood samples at equal spaces along a 10-centimeter length was shown to be feasible and safe in patients undergoing angioplasty. In unobstructed vessels with no lesion, the investigators observed no gradients of the 92 biomolecules chosen for multiplexed analysis. By contrast, stable and disrupted plaques exhibited biomolecule gradients along the sampling length, implying the release of substances from plaques into the boundary layer of the vessel, and that flowing blood was coursing over them. The investigators detected several gradients likely derived from the endothelium overlying plaques, particularly the oxidized low-density lipoprotein (LDL) receptor (OLR1, also known as LOX-1), as well as inflammatory mediators, consistent with the inflammatory status of endothelium.
After angioplasty, some molecular gradients persisted, though the investigators observed the release of additional substances. One of the most notable released substances was matrix metalloproteinase-12 (MMP12), which is normally undetectable in endothelial cells or smooth muscle cells and is expressed only around the core of vulnerable plaques. Due to the causative role of MMP12 in early strokes and its association with subsequent strokes and major adverse events, the investigators surmised that the post-angioplasty gradient of MMP12 may yield important diagnostic or prognostic information.
MedicalResearch.com: What should readers take away from your report?
- The PlaqueTec Liquid Biopsy System (LBS) is a disruptive technology; a first-in-class dedicated coronary blood sampling device, that overcomes the shortcomings of generic microcatheters and samples directly from the boundary layer within the coronary artery at 4 spatially-separated sites simultaneously.
- Gradients of biomolecules have been discovered across coronary plaques in vivo, with differential expression of such molecules observed in different disease states – little or no biomarker release was observed in unobstructed vessels; increased levels of platelet, monocyte and endothelial cell markers in stable obstructive plaques; and elevations in macrophage/lymphocyte markers as well as plaque core constituents after iatrogenic balloon injury (before stenting).
- Such plaque-level individual patient data may pave the way to aiding patient risk stratification, re-tasking of existing anti-inflammatory biologic agents, identification of novel inflammatory targets not detectable in peripheral blood and the de-risking future early-stage studies of novel pharmaceutical agents.
MedicalResearch.com: What recommendations do you have for future research as a result of this study?
Response: Further avenues for future research work include determining the relationship between indices of systemic inflammation with local/coronary inflammation, and also the morphology of the candidate coronary plaque; examination of other aspects of the atherosclerotic process, including thrombosis and vascular calcification, at the intracoronary/transplaque level; and examining different patient subgroups to determine whether key differences exist that may assist tailoring of therapies aimed at modulating individual patients’ prognosis.
MedicalResearch.com: Is there anything else you would like to add?
Response: Historically, with the well-defined anti-inflammatory characteristics of statins, teasing out the contribution of reducing inflammation over and above that of cholesterol reduction in attenuating future events has been tricky. The recently-published CANTOS study (Ridker P et al. N Engl J Med 2017; 377: 1119-1131) has produced the first evidence that targeting inflammation independently can reduce major adverse cardiac events in patients with prior myocardial infarction/heart attack, allowing clinicians an important alternative route to mitigate patients’ future risk. This said, identifying patients at risk remains controversial owing to the complex interaction between peripheral inflammation, coronary inflammation and coronary plaque phenotype, all of which have been implicated in future risk of adverse events.
Therefore, identification of a local inflammatory milieu within the coronary artery itself could yield very important information to help stratify patients at risk, and to guide tailoring of specific therapies designed to improve individuals’ prognosis.
The only disclosure I have is that my role as PlaqueTec Chief Medical Officer is as a consultant.
Citations:
Percutaneous Sampling of Local Biomolecule Gradients Across Coronary Artery Atherosclerotic Plaques
Nick E.J. West, Joseph P. Corrigan, Richard H.G. Owen, Stephen P. Hoole, Adam J. Brown, Stephen Blatcher, Andrew C. Newby
JACC: Basic to Translational Science December 01, 2017, 2 (6) 646-654; DOI: 10.1016/j.jacbts.2017.07.007
MedicalResearch.com is not a forum for the exchange of personal medical information, advice or the promotion of self-destructive behavior (e.g., eating disorders, suicide). While you may freely discuss your troubles, you should not look to the Website for information or advice on such topics. Instead, we recommend that you talk in person with a trusted medical professional.
The information on MedicalResearch.com is provided for educational purposes only, and is in no way intended to diagnose, cure, or treat any medical or other condition. Always seek the advice of your physician or other qualified health and ask your doctor any questions you may have regarding a medical condition. In addition to all other limitations and disclaimers in this agreement, service provider and its third party providers disclaim any liability or loss in connection with the content provided on this website.
Last Updated on January 16, 2018 by Marie Benz MD FAAD