MedicalResearch.com Interview with:
[caption id="attachment_53245" align="alignleft" width="143"]

Dr. Tymianski[/caption]
Michael Tymianski, CM, MD, PhD, FRCSC, FAHA
Head, Division of Neurosurgery, University Health Network
Medical Director, Neurovascular Therapeutics Program, University Health Network
Professor, Departments of Surgery and Physiology, University of Toronto
Senior Scientist, Toronto Western Hospital Research Institute
Director, Neuroprotection Laboratory, Toronto Western Hospital
President and CEO, NoNO Inc
MedicalResearch.com: What is the background for this study? How is alteplase related to and affect nerinetide?
Response: Cerebral neuroprotection for acute ischemic stroke (AIS) is defined as a therapy aimed at enhancing the brain’s resilience to ischemia to improve the clinical outcome of affected individuals. Although traditionally aimed at the salvage of neurons, this term may be equally applicable to all the cellular constituents of the brain, including cells of cerebral blood vessels, neurons, and glia. Pharmacological neuroprotection (hereafter referred to as neuroprotection) would be achieved by drugs targeting one or more critical components of the ischemic cascade that lead to ischemic damage. The feasibility of neuroprotection has a strong basis in animal experiments, but research for several decades has failed to translate neuroprotective treatments from animals to humans. The disappointing results of all controlled clinical neuroprotection trials for AIS have cast doubts as to whether neuroprotection in humans is biologically possible and, given the complexities of human stroke syndromes, whether it is a clinically practicable therapy for patients experiencing AIS in the community.
In the case of neuroprotection trials for acute ischemic stroke, all to date have failed to demonstrate a clinical benefit of the study agent. Our review of studies since the year 2000 shows that many were not conducted in accordance with the animal studies that supported efficacy. They enrolled a heterogeneous subject population with varying (small and large) vessel occlusions and without knowledge of the degree of completed infarctions. Most had not implemented a strategy to ensure that the treatment effect size was maximized, and all in-hospital trials enrolled in treatment windows that exceeded 4 hours, at which an important proportion of enrolled subjects cannot respond to treatment because they no longer have salvageable brain.
The ESCAPE-NA1 addressed past deficiencies of AIS trials. It was based on a sound scientific foundation including extensive animal studies, and capitalized on the designs that led to success in AIS trials of endovascular thrombectomy. ESCAPE-NA1 enrolled patients proven by these past trials to have salvageable brain at the time that the treatment was given, and tested the drug in an ischemia-reperfusion scenario in which it was anticipated to be most effective. The enrollment was over 12 hours, but only including patients who had medical imaging suggestive that they still had salvageable brain.
Alteplase is an agent that activates the protease plasmin in the bloodstream. Plasmin cleaves peptides at certain spots within their structure, and it is a known biological fact that plasmin is able to cleave nerinetide. What was not known at the time of the trial was the degree to which this would reduce nerinetide plasma leves in humans, and the impact that this would have on the therapeutic effects of nerinetide. This is why we conducted a very large trial in which the participants’ enrollment was stratified according to whether or not they received alteplase. This ensured that there was good balance within each stratum, thereby enabling us to make more robust conclusions.








 Dr. Curhan[/caption]
Sharon G. Curhan, MD, ScM|
Director, CHEARS: The Conservation of Hearing Study
Channing Division of Network Medicine
Department of Medicine
Brigham and Women’s Hospital
Harvard Medical School
Boston, MA 02114
MedicalResearch.com: What is the background for this study?
Response: Herpes zoster, commonly known as “shingles,” is a viral infection that often causes a painful rash. Shingles can occur anywhere on the head or body. Shingles is caused by the varicella zoster virus (VZV), the same virus that causes chickenpox. After a person has chickenpox, the virus stays in their body for the rest of their life. Years and even decades later, the virus may reactivate as shingles. Almost all individuals age 50 years and older in the US have been infected with the varicella zoster virus and therefore they are at risk for shingles.
About 1 in 3 people will develop shingles during their lifetime, and since age is a risk factor for shingles, this number may increase as the population ages. The risk is also higher among individuals of any age who are immunocompromised due to disease or treatment. A number of serious complications can occur when a person develops shingles, such as post-herpetic neuralgia (long-lasting pain), but there was limited information on whether there are other adverse long-term health implications of developing shingles.
There is a growing body of evidence that links VZV, the virus that causes shingles, to vascular disease. VZV vasculopathy may cause damage to blood vessels and increase the risk of stroke or coronary heart disease. Although some previous studies showed a higher risk of stroke or heart attack around the time of the shingles infection, it was not known whether this higher risk persisted in the long term. Therefore, the question we aimed to address in this study was to investigate whether shingles is associated with higher long-term risk of stroke or coronary heart disease.
To address this question, we conducted a prospective longitudinal study in 3 large US cohorts of >200,000 women and men, the Nurses’ Health Study (>79,000 women), the Nurses’ Health Study II (almost 94,000 women) and the Health Professionals Follow-Up Study (>31,000 men), without a prior history of stroke or coronary heart disease. We collected information on shingles, stroke and coronary heart disease on biennial questionnaires and confirmed the diagnoses with medical record review. We followed the participants for up to 16 years and evaluated whether those who had developed shingles were at higher risk for stroke or coronary heart disease years after the shingles episode. The outcomes we measured were incident stroke, incident coronary heart disease [defined as having a non-fatal or fatal myocardial infarction (heart attack) or a coronary revascularization procedure (CABG, coronary artery bypass graft or percutaneous transluminal coronary angioplasty)]. We also evaluated a combined outcome of cardiovascular disease, which included either stroke or coronary heart disease, whichever came first.
Dr. Curhan[/caption]
Sharon G. Curhan, MD, ScM|
Director, CHEARS: The Conservation of Hearing Study
Channing Division of Network Medicine
Department of Medicine
Brigham and Women’s Hospital
Harvard Medical School
Boston, MA 02114
MedicalResearch.com: What is the background for this study?
Response: Herpes zoster, commonly known as “shingles,” is a viral infection that often causes a painful rash. Shingles can occur anywhere on the head or body. Shingles is caused by the varicella zoster virus (VZV), the same virus that causes chickenpox. After a person has chickenpox, the virus stays in their body for the rest of their life. Years and even decades later, the virus may reactivate as shingles. Almost all individuals age 50 years and older in the US have been infected with the varicella zoster virus and therefore they are at risk for shingles.
About 1 in 3 people will develop shingles during their lifetime, and since age is a risk factor for shingles, this number may increase as the population ages. The risk is also higher among individuals of any age who are immunocompromised due to disease or treatment. A number of serious complications can occur when a person develops shingles, such as post-herpetic neuralgia (long-lasting pain), but there was limited information on whether there are other adverse long-term health implications of developing shingles.
There is a growing body of evidence that links VZV, the virus that causes shingles, to vascular disease. VZV vasculopathy may cause damage to blood vessels and increase the risk of stroke or coronary heart disease. Although some previous studies showed a higher risk of stroke or heart attack around the time of the shingles infection, it was not known whether this higher risk persisted in the long term. Therefore, the question we aimed to address in this study was to investigate whether shingles is associated with higher long-term risk of stroke or coronary heart disease.
To address this question, we conducted a prospective longitudinal study in 3 large US cohorts of >200,000 women and men, the Nurses’ Health Study (>79,000 women), the Nurses’ Health Study II (almost 94,000 women) and the Health Professionals Follow-Up Study (>31,000 men), without a prior history of stroke or coronary heart disease. We collected information on shingles, stroke and coronary heart disease on biennial questionnaires and confirmed the diagnoses with medical record review. We followed the participants for up to 16 years and evaluated whether those who had developed shingles were at higher risk for stroke or coronary heart disease years after the shingles episode. The outcomes we measured were incident stroke, incident coronary heart disease [defined as having a non-fatal or fatal myocardial infarction (heart attack) or a coronary revascularization procedure (CABG, coronary artery bypass graft or percutaneous transluminal coronary angioplasty)]. We also evaluated a combined outcome of cardiovascular disease, which included either stroke or coronary heart disease, whichever came first.


 Dr. Smyth[/caption]
Professor Andrew Smyth MB, BCh, BAO, MMedSc, MRCPI, PhD
Professor of Clinical Epidemiology
NUI Galway
Director of the HRB-Clinical Research Facility Galway
Consultant Nephrologist at Galway University Hospitals
MedicalResearch.com: What is the background for this study?
Response: We know that there are multiple medium to long-term risk factors for stroke, as people with conditions such as hypertension (high blood pressure) or diabetes mellitus (high blood glucose levels) and those with risk factors (such as smoking, obesity, poor diet quality and others) are at increased risk of stroke. However, we still find it difficult to predict who will have a stroke.
We were interested in exploring if short-term exposures to anger or emotional upset or a period of heavy physical exertion might lead to, or ‘trigger’ a stroke. We looked at this previously for myocardial infarction (heart attack) in a study called INTERHEART. Some smaller studies have looked at this before, with less people experiencing a stroke and often confined to one country or geographical region. Here, in INTERSTROKE, we included over 13,000 people who had a stroke and asked about the one hour period before the onset of the stroke and also about the same period on the day before.
Dr. Smyth[/caption]
Professor Andrew Smyth MB, BCh, BAO, MMedSc, MRCPI, PhD
Professor of Clinical Epidemiology
NUI Galway
Director of the HRB-Clinical Research Facility Galway
Consultant Nephrologist at Galway University Hospitals
MedicalResearch.com: What is the background for this study?
Response: We know that there are multiple medium to long-term risk factors for stroke, as people with conditions such as hypertension (high blood pressure) or diabetes mellitus (high blood glucose levels) and those with risk factors (such as smoking, obesity, poor diet quality and others) are at increased risk of stroke. However, we still find it difficult to predict who will have a stroke.
We were interested in exploring if short-term exposures to anger or emotional upset or a period of heavy physical exertion might lead to, or ‘trigger’ a stroke. We looked at this previously for myocardial infarction (heart attack) in a study called INTERHEART. Some smaller studies have looked at this before, with less people experiencing a stroke and often confined to one country or geographical region. Here, in INTERSTROKE, we included over 13,000 people who had a stroke and asked about the one hour period before the onset of the stroke and also about the same period on the day before.
 Dr. Singer[/caption]
Daniel E. Singer, MD
Professor of Medicine, Harvard Medical School
Professor in the Department of Epidemiology
Harvard T.H. Chan School of Public Health
Division of General Internal Medicine
Massachusetts General Hospital
Boston, MA, 02114
MedicalResearch.com: What is the background for this study?
Response: Atrial fibrillation (AF) raises the risk of ischemic stroke 4-5-fold and this risk is largely reversible by oral anticoagulants (OAC). These facts are part of the core knowledge of internal medicine and the basis of multiple guidelines. They are based on studies of patients with persistent or predominantly “heavy burden” paroxysmal AF completed in the 1990s.
More recent studies using cardiac implantable devices (CIEDs: implantable defibrillators, pacemakers, etc) which have the capacity to monitor heart rhythm continuously have found that many older patients have brief, often undiagnosed, episodes of AF. Several of these studies have found that strokes occur during periods of sinus rhythm temporally distant from a preceding episode of AF. This has led to a widespread suspicion that AF is not a direct causal risk factor but a risk “marker” indicating the presence of other truly causal features like a diseased left atrium (atrial myopathy). If the risk marker hypothesis is correct, then long-term anticoagulation is needed even for brief and rare episodes of AF (assuming the patient’ s CHA2DS2-VASc score is high enough). The key problem with prior prospective studies using CIEDs was that only a small number of strokes were observed leading to inadequate statistical power.
Our study addressed this power problem by linking the very large Optum electronic health record database which could identify ischemic strokes with the Medtronic CareLink database of long-term, continuous heart rhythm records of patients with CIEDs. We ended up studying 891 individuals who had an ischemic stroke and had 120 days of continuous heart monitoring prior to the stroke.
Dr. Singer[/caption]
Daniel E. Singer, MD
Professor of Medicine, Harvard Medical School
Professor in the Department of Epidemiology
Harvard T.H. Chan School of Public Health
Division of General Internal Medicine
Massachusetts General Hospital
Boston, MA, 02114
MedicalResearch.com: What is the background for this study?
Response: Atrial fibrillation (AF) raises the risk of ischemic stroke 4-5-fold and this risk is largely reversible by oral anticoagulants (OAC). These facts are part of the core knowledge of internal medicine and the basis of multiple guidelines. They are based on studies of patients with persistent or predominantly “heavy burden” paroxysmal AF completed in the 1990s.
More recent studies using cardiac implantable devices (CIEDs: implantable defibrillators, pacemakers, etc) which have the capacity to monitor heart rhythm continuously have found that many older patients have brief, often undiagnosed, episodes of AF. Several of these studies have found that strokes occur during periods of sinus rhythm temporally distant from a preceding episode of AF. This has led to a widespread suspicion that AF is not a direct causal risk factor but a risk “marker” indicating the presence of other truly causal features like a diseased left atrium (atrial myopathy). If the risk marker hypothesis is correct, then long-term anticoagulation is needed even for brief and rare episodes of AF (assuming the patient’ s CHA2DS2-VASc score is high enough). The key problem with prior prospective studies using CIEDs was that only a small number of strokes were observed leading to inadequate statistical power.
Our study addressed this power problem by linking the very large Optum electronic health record database which could identify ischemic strokes with the Medtronic CareLink database of long-term, continuous heart rhythm records of patients with CIEDs. We ended up studying 891 individuals who had an ischemic stroke and had 120 days of continuous heart monitoring prior to the stroke. 
 Dr. Tian[/caption]
MedicalResearch.com Interview with:
Maoyi TIAN PhD
Program Head, Digital Health and Head, Injury & Trauma
Senior Research Fellow
The George Institute
MedicalResearch.com: What is the background for this study?
Response: There is clear evidence from the literature that sodium reduction or potassium supplementation can reduce blood pressure. Reduced blood pressure can also lead to a risk reduction for cardiovascular diseases.
Salt substitute is a reduced sodium added potassium product combined those effects. Previous research of salt substitute focus on the blood pressure outcome. There is no evidence if salt substitute can reduce the risk of cardiovascular diseases or pre-mature death. This study provided a definitive evidence for this unaddressed question.
MedicalResearch.com: What are the main findings?
The main findings of the research were:
Dr. Tian[/caption]
MedicalResearch.com Interview with:
Maoyi TIAN PhD
Program Head, Digital Health and Head, Injury & Trauma
Senior Research Fellow
The George Institute
MedicalResearch.com: What is the background for this study?
Response: There is clear evidence from the literature that sodium reduction or potassium supplementation can reduce blood pressure. Reduced blood pressure can also lead to a risk reduction for cardiovascular diseases.
Salt substitute is a reduced sodium added potassium product combined those effects. Previous research of salt substitute focus on the blood pressure outcome. There is no evidence if salt substitute can reduce the risk of cardiovascular diseases or pre-mature death. This study provided a definitive evidence for this unaddressed question.
MedicalResearch.com: What are the main findings?
The main findings of the research were:


 Dr. Fornwalt[/caption]
Brandon K Fornwalt, MD, PhD
Associate Professor, Director Department of Imaging Science and Innovation
Geisinger
MedicalResearch.com: What is the background for this study?
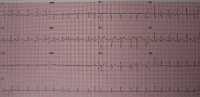
Response: Atrial fibrillation (AF) is an abnormal heart rhythm that is associated with outcomes such as stroke, heart failure and death. If we know a patient has atrial fibrillation, we can treat them to reduce the risk of stroke by nearly two-thirds. Unfortunately, patients often don’t know they have AF. They present initially with a stroke, and we have no chance to treat them before this happens. If we could predict who is at high risk of either currently having AF or developing it in the near future, we could intervene earlier and hopefully reduce bad outcomes like stroke. Artificial intelligence approaches may be able to help with this task.
Dr. Fornwalt[/caption]
Brandon K Fornwalt, MD, PhD
Associate Professor, Director Department of Imaging Science and Innovation
Geisinger
MedicalResearch.com: What is the background for this study?
Response: Atrial fibrillation (AF) is an abnormal heart rhythm that is associated with outcomes such as stroke, heart failure and death. If we know a patient has atrial fibrillation, we can treat them to reduce the risk of stroke by nearly two-thirds. Unfortunately, patients often don’t know they have AF. They present initially with a stroke, and we have no chance to treat them before this happens. If we could predict who is at high risk of either currently having AF or developing it in the near future, we could intervene earlier and hopefully reduce bad outcomes like stroke. Artificial intelligence approaches may be able to help with this task. 










 Kazuo Kitagawa, MD PhD
Department of Neurology
Tokyo Women's Medical University
Tokyo, Japan
MedicalResearch.com: What is the background for this study? What are the main findings
Response: Reduction in blood pressure (BP) reduces the rates of recurrent stroke, but the optimum BP target remained unclear.
The results of RESPECT Study together with up-dated meta-analysis showed the benefit of intensive blood pressure lowering (<130/80 mmHg) compared with standard BP lowering (<140/90 mmHg).
Kazuo Kitagawa, MD PhD
Department of Neurology
Tokyo Women's Medical University
Tokyo, Japan
MedicalResearch.com: What is the background for this study? What are the main findings
Response: Reduction in blood pressure (BP) reduces the rates of recurrent stroke, but the optimum BP target remained unclear.
The results of RESPECT Study together with up-dated meta-analysis showed the benefit of intensive blood pressure lowering (<130/80 mmHg) compared with standard BP lowering (<140/90 mmHg). 


