

10 Aug UPenn Dental Research: Antiviral and Antibacterial Chewing Gum Targets HPV and Oral Pathogens Linked to Head and Neck Cancer
MedicalResearch.com Interview with:
Henry Daniell, PhD
Vice-Chair and W.D. Miller Professor
Department of Basic & Translational Sciences
School of Dental Medicine, University of Pennsylvania, Philadelphia PA
Dr. Henry Daniell, Ph.D.[/caption]
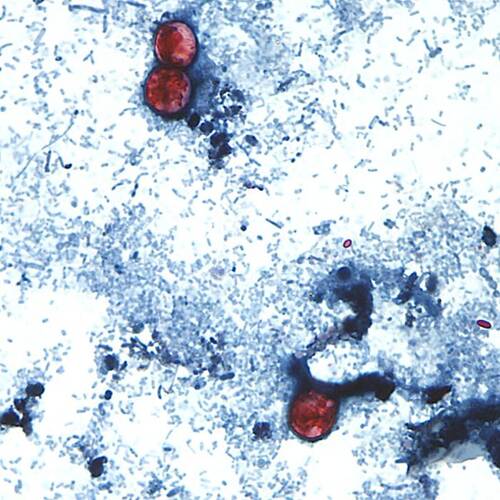
MedicalResearch.com: What is the background for this study? What bacteria or viruses are associated with head and neck squamous cell carcinomas?
Dr. Daniell: Human Papilloma Virus (HPV), anaerobic bacteria Porphyromonas gingivalis (Pg) and Fusobacterium nucleatum (Fn) correlate with worse survival of head and neck squamous cell carcinoma (HNSCC). In tumorigenic cells HPV genome integrates into the host cell genome causing genome instability and genic alteration which facilitate mutation and hyperproliferation. One third of males in the globe is HPV positive and one fifth are infected with high risk HPV16 strain. Pg is invasive and replicates within tumor cells and influences oncogenic signaling of HNSCC. Fn triggers cancer progression by upregulating several oncogenes responsible for inflammation, cell proliferation, invasion, metastasis. Therefore, it is important to control HPV, Pg, and Fn in the oral cavity to reduce initiation or advancement of oral cancer.

 Dr. Adalja[/caption]
Dr. Adalja[/caption]











 Candida auris CDC Image[/caption]
MedicalResearch.com Interview with:
[caption id="attachment_72627" align="alignleft" width="200"]
Candida auris CDC Image[/caption]
MedicalResearch.com Interview with:
[caption id="attachment_72627" align="alignleft" width="200"]

 Dr. Schaffner[/caption]
William Schaffner, MD
Dr. Schaffner[/caption]
William Schaffner, MD
 MedicalResearch.com: What roles do a decrease in US immunization rates and/or increased immigration from under-vaccinated area play in this increase?
Response: The substantial majority of unimmunized children in the US were born and raised in this country. They usually are members of middle- or upper-income families. The most frequent importers of measles into the US are our own unimmunized children who travel abroad, encounter measles virus and bring it back to their homes where the virus then spreads among the child’s schoolmates and playmates, creating an outbreak.
MedicalResearch.com: What roles do a decrease in US immunization rates and/or increased immigration from under-vaccinated area play in this increase?
Response: The substantial majority of unimmunized children in the US were born and raised in this country. They usually are members of middle- or upper-income families. The most frequent importers of measles into the US are our own unimmunized children who travel abroad, encounter measles virus and bring it back to their homes where the virus then spreads among the child’s schoolmates and playmates, creating an outbreak.
 Dr. Freedman M.D.[/caption]
David O. Freedman, M.D.
Professor Emeritus of Infectious Diseases
Editor of the Textbook of Travel Medicine
World Health Organization—Member, Emergency Committee on Zika Virus
University of Alabama, Birmingham USA
MedicalResearch.com: What is the background for this outbreak?
Response: India has reported 2 confirmed (PCR and ELISA) Nipah virus (NiV) cases in West Bengal State where the Kolkata megalopolis is located; the state borders Bangladesh. Symptom onset in both cases was late December 2025 in 2 health care workers. One patient has improved while the other remains in the ICU. All samples from 200 contact persons tested negative for NiV. No further confirmed cases have been detected in West Bengal
Bangladesh has reported 1 confirmed NiV case in Rajshahi Division which neighbors India. Symptom onset was January 21, 2026, and the patient expired on January 28. The patient reported no travel history but reported repeated consumption of raw date palm sap between 5 and 20 January. All 35 contact-persons are being monitored and have tested negative for NiV and no further cases have been detected to date.
Dr. Freedman M.D.[/caption]
David O. Freedman, M.D.
Professor Emeritus of Infectious Diseases
Editor of the Textbook of Travel Medicine
World Health Organization—Member, Emergency Committee on Zika Virus
University of Alabama, Birmingham USA
MedicalResearch.com: What is the background for this outbreak?
Response: India has reported 2 confirmed (PCR and ELISA) Nipah virus (NiV) cases in West Bengal State where the Kolkata megalopolis is located; the state borders Bangladesh. Symptom onset in both cases was late December 2025 in 2 health care workers. One patient has improved while the other remains in the ICU. All samples from 200 contact persons tested negative for NiV. No further confirmed cases have been detected in West Bengal
Bangladesh has reported 1 confirmed NiV case in Rajshahi Division which neighbors India. Symptom onset was January 21, 2026, and the patient expired on January 28. The patient reported no travel history but reported repeated consumption of raw date palm sap between 5 and 20 January. All 35 contact-persons are being monitored and have tested negative for NiV and no further cases have been detected to date.



 Dr. Dehghani[/caption]
MedicalResearch.com Interview with:
Ali Dehghani, DO
Department of Medicine
University Hospitals Cleveland Medical Center / Case Western Reserve University
Presenting Author, IDWeek 2025
MedicalResearch.com: What is the background for this study?
Response: Shingles (herpes zoster) is caused by reactivation of the varicella-zoster virus, which can inflame blood vessels and the nervous system. Evidence over the past decade has linked shingles to higher risks of heart attack, stroke, and dementia—but it was unclear whether the shingles vaccine might lessen those long-term effects.
[caption id="attachment_71061" align="aligncenter" width="500"]
Dr. Dehghani[/caption]
MedicalResearch.com Interview with:
Ali Dehghani, DO
Department of Medicine
University Hospitals Cleveland Medical Center / Case Western Reserve University
Presenting Author, IDWeek 2025
MedicalResearch.com: What is the background for this study?
Response: Shingles (herpes zoster) is caused by reactivation of the varicella-zoster virus, which can inflame blood vessels and the nervous system. Evidence over the past decade has linked shingles to higher risks of heart attack, stroke, and dementia—but it was unclear whether the shingles vaccine might lessen those long-term effects.
[caption id="attachment_71061" align="aligncenter" width="500"]



