

24 Mar Karolinska Institutet Study Finds APOE Genotype Influences Link Between Red Meat Consumption and Cognitive Decline
Posted at 23:42h
in Alzheimer's - Dementia, Author Interviews, Genetic Research, JAMA, Karolinski Institute
[caption id="attachment_72900" align="alignleft" width="200"] Jakob Norgren, Ph.D.[/caption]
MedicalResearch.com Interview with:
Jakob Norgren | PhD, Postdoctoral Researcher
Department of Neurobiology, Care Sciences and Society (NVS) | Karolinska Institutet
Division of Clinical Geriatrics | Center for Alzheimer Research
Huddinge, Sweden
MedicalResearch.com: What is the background for this study?
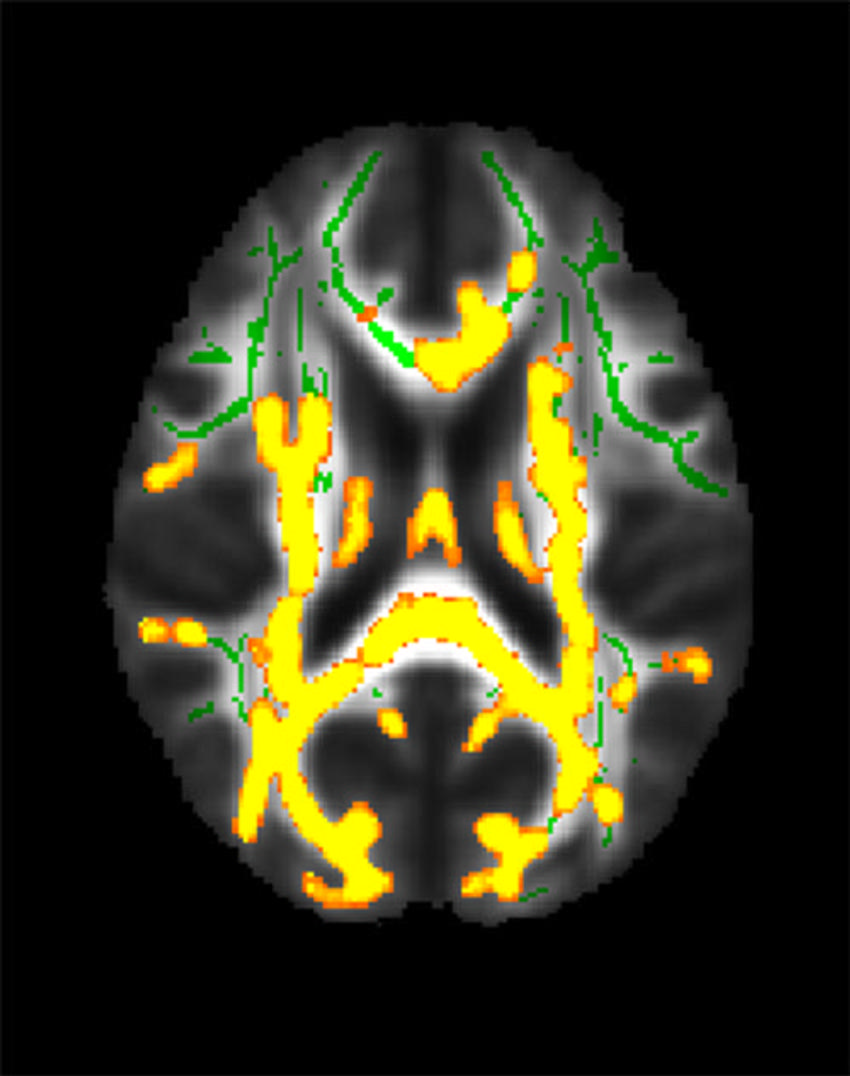
Response: This study tested the hypothesis that people with APOE 3/4 and 4/4 would have a reduced risk of cognitive decline and dementia with higher meat intake, based on the fact that APOE4 is the evolutionarily oldest variant of the APOE gene and may have arisen during a period when our evolutionary ancestors ate a more animal-based diet.














 Dr. Guasch-Ferré[/caption]
Marta Guasch-Ferré, PhD
Associate Professor and Deputy Head of Section, Section of Epidemiology
University of Copenhagen
Group Leader, Novo Nordisk Foundation Center for Basic Metabolic Research
Adjunct Associate Professor, Department of Nutrition
Harvard TH Chan School of Public Health
MedicalResearch.com: What is the background for this study?
Response: Olive oil is rich in monounsaturated fats and contains compounds with antioxidant activity that may play a protective role for the brain. Olive oil as part of a Mediterranean diet appears to have a beneficial effect against cognitive decline. Higher olive oil intake was previously associated with a lower risk of cardiovascular disease and mortality. But its association with dementia mortality was unknown.
Dr. Guasch-Ferré[/caption]
Marta Guasch-Ferré, PhD
Associate Professor and Deputy Head of Section, Section of Epidemiology
University of Copenhagen
Group Leader, Novo Nordisk Foundation Center for Basic Metabolic Research
Adjunct Associate Professor, Department of Nutrition
Harvard TH Chan School of Public Health
MedicalResearch.com: What is the background for this study?
Response: Olive oil is rich in monounsaturated fats and contains compounds with antioxidant activity that may play a protective role for the brain. Olive oil as part of a Mediterranean diet appears to have a beneficial effect against cognitive decline. Higher olive oil intake was previously associated with a lower risk of cardiovascular disease and mortality. But its association with dementia mortality was unknown.

 Dr. Li Gan[/caption]
Dr. Li Gan PhD
Burton P. and Judith B. Resnick Distinguished Professor in Neurodegenerative Diseases
Brain and Mind Research Institute
Weill Cornell Medical College
[caption id="attachment_61627" align="alignleft" width="150"]
Dr. Li Gan[/caption]
Dr. Li Gan PhD
Burton P. and Judith B. Resnick Distinguished Professor in Neurodegenerative Diseases
Brain and Mind Research Institute
Weill Cornell Medical College
[caption id="attachment_61627" align="alignleft" width="150"]
 Dr. Dolatshahi[/caption]
Mahsa Dolatshahi, M.D., M.P.H.
Post-doctoral research fellow
Mallinckrodt Institute of Radiology (MIR)
Washington University School of Medicine
St. Louis
MedicalResearch.com: What is the background for this study?
Response: Obesity at midlife is recognized as a risk factor for developing Alzheimer disease decades afterwards. However, body mass index on its own does not adequately represent the risks associated with obesity.
In this study, we went beyond BMI and considered anatomical distribution of body fat, including the metabolically active visceral fat in the belly, and showed its association with Alzheimer pathology in the form of amyloid proteins. In addition, visceral fat along with obesity and insulin resistance were associated with thinning of brain cortex, as early as midlife.
Dr. Dolatshahi[/caption]
Mahsa Dolatshahi, M.D., M.P.H.
Post-doctoral research fellow
Mallinckrodt Institute of Radiology (MIR)
Washington University School of Medicine
St. Louis
MedicalResearch.com: What is the background for this study?
Response: Obesity at midlife is recognized as a risk factor for developing Alzheimer disease decades afterwards. However, body mass index on its own does not adequately represent the risks associated with obesity.
In this study, we went beyond BMI and considered anatomical distribution of body fat, including the metabolically active visceral fat in the belly, and showed its association with Alzheimer pathology in the form of amyloid proteins. In addition, visceral fat along with obesity and insulin resistance were associated with thinning of brain cortex, as early as midlife.

 Dr. Belloy[/caption]
Michael E. Belloy, PhD
Department of Neurology and Neurological Sciences
Stanford University, Stanford, California
MedicalResearch.com: What is the background for this study?
Response: Apolipoprotein E (APOE)*2 and APOE*4 are, respectively, the strongest protective and risk-increasing, genetic variants for late-onset Alzheimer disease. As such, one’s APOE genotype is highly relevant towards clinical trial design and Alzheimer’s disease research. However, most insights so far are focused on the associations of these APOE genotypes with Alzheimer’s disease risk in non-Hispanic white individuals.
One important aspect of our work is that we really increased sample sizes for non-Hispanic Black, Hispanic, and East Asian individuals, so that we now have better understanding of the associations of APOE genotypes with Alzheimer’s disease risk in these groups. In complement, we also did the largest investigation to date on the role of ancestry on the associations of APOE genotypes with Alzheimer’s disease risk. The scale of our study was thus a critical factor in generating novel insights.
Dr. Belloy[/caption]
Michael E. Belloy, PhD
Department of Neurology and Neurological Sciences
Stanford University, Stanford, California
MedicalResearch.com: What is the background for this study?
Response: Apolipoprotein E (APOE)*2 and APOE*4 are, respectively, the strongest protective and risk-increasing, genetic variants for late-onset Alzheimer disease. As such, one’s APOE genotype is highly relevant towards clinical trial design and Alzheimer’s disease research. However, most insights so far are focused on the associations of these APOE genotypes with Alzheimer’s disease risk in non-Hispanic white individuals.
One important aspect of our work is that we really increased sample sizes for non-Hispanic Black, Hispanic, and East Asian individuals, so that we now have better understanding of the associations of APOE genotypes with Alzheimer’s disease risk in these groups. In complement, we also did the largest investigation to date on the role of ancestry on the associations of APOE genotypes with Alzheimer’s disease risk. The scale of our study was thus a critical factor in generating novel insights.




 Dr. Manson[/caption]
JoAnn E. Manson, MD, DrPH, MACP
Dr. Manson[/caption]
JoAnn E. Manson, MD, DrPH, MACP


 Julia Cave Arbanas[/caption]
Julia Cave Arbanas
Project Manager and
Julia Cave Arbanas[/caption]
Julia Cave Arbanas
Project Manager and




 Dr. Martens[/caption]
Christopher R. Martens PhD
Assistant Professor
Director, Delaware Center for Cognitive Aging Research
Department of Kinesiology & Applied Physiology
University of Delaware
Newark, DE
MedicalResearch.com: What is the background for this study?
Response: One of the main issues with Alzheimer's disease is an impaired ability to make energy in the brain. NAD+ is critically involved in the creation of energy within cells and there is strong evidence that nicotinamide riboside (NR), a precursor to NAD+, can restore brain function in mice that exhibit similar characteristics as people with Alzheimer's disease.
We had previously studied the effects of NR in healthy older adults and wanted to see whether it is even capable of getting into brain tissue. We used remaining blood samples from our original study and measured the amount of NAD+ within tiny "vesicles" in the blood that we are quite confident originated from the brain and other neural tissue
Dr. Martens[/caption]
Christopher R. Martens PhD
Assistant Professor
Director, Delaware Center for Cognitive Aging Research
Department of Kinesiology & Applied Physiology
University of Delaware
Newark, DE
MedicalResearch.com: What is the background for this study?
Response: One of the main issues with Alzheimer's disease is an impaired ability to make energy in the brain. NAD+ is critically involved in the creation of energy within cells and there is strong evidence that nicotinamide riboside (NR), a precursor to NAD+, can restore brain function in mice that exhibit similar characteristics as people with Alzheimer's disease.
We had previously studied the effects of NR in healthy older adults and wanted to see whether it is even capable of getting into brain tissue. We used remaining blood samples from our original study and measured the amount of NAD+ within tiny "vesicles" in the blood that we are quite confident originated from the brain and other neural tissue