
12 Feb Parkinson’s Disease-specific imaging: Enhancing precision in CNS clinical trials
[caption id="attachment_72368" align="aligncenter" width="500"] Freepix[/caption]
 Freepix[/caption]
Freepix[/caption]
 Dr. Fyfe[/caption]
Dr. Caroline Fyfe PhD
Postdoctoral Research Associate
Life Long Health and Wellbeing Theme
University of Edinburgh
MedicalResearch.com: What is the background for this study?
Response: Autism (ASD) has traditionally been seen as a condition that disproportionately affects males. This study quantifies the sex bias across birth cohorts, ages, and calendar time, using the Swedish national population registers to follow ~ 2.7 million individual born between 1985 and 2020 throughout their lives. Among children under ten years old the male-to-female diagnosis ratio remained relatively stable at about 3:1.
In contrast, a rapid increase in diagnoses of ASD among females during adolescence, produced a “female catch-up effect” that resulted in near parity of ASD prevalence between males and females by adulthood.
Dr. Fyfe[/caption]
Dr. Caroline Fyfe PhD
Postdoctoral Research Associate
Life Long Health and Wellbeing Theme
University of Edinburgh
MedicalResearch.com: What is the background for this study?
Response: Autism (ASD) has traditionally been seen as a condition that disproportionately affects males. This study quantifies the sex bias across birth cohorts, ages, and calendar time, using the Swedish national population registers to follow ~ 2.7 million individual born between 1985 and 2020 throughout their lives. Among children under ten years old the male-to-female diagnosis ratio remained relatively stable at about 3:1.
In contrast, a rapid increase in diagnoses of ASD among females during adolescence, produced a “female catch-up effect” that resulted in near parity of ASD prevalence between males and females by adulthood.
 Hermona Soreq, lab, students, collaboration[/caption]
Prof. Hermona Soreq
The Edmond and Lily Safra Center for Brain Sciences (ELSC) and
The Alexander Silberman Institute of Life Science
at the Hebrew University
MedicalResearch.com: What is the background for this study? What are tRFs and how do they impact neurodegeneration?
Hermona Soreq, lab, students, collaboration[/caption]
Prof. Hermona Soreq
The Edmond and Lily Safra Center for Brain Sciences (ELSC) and
The Alexander Silberman Institute of Life Science
at the Hebrew University
MedicalResearch.com: What is the background for this study? What are tRFs and how do they impact neurodegeneration?

Diagnostic Biochips leverages advanced neural probes to enhance neuroscience research. These advanced probes, combined with AI-powered data analysis, offer precise insights into neurological disorders such as Alzheimer's and Parkinson's....
 Dr. Gus Alva[/caption]
Gus Alva, MD, DFAPA
Medical Director, ATP Clinical Research
Medical Director, Senior Brain Health, Hoag Hospital, Newport Beach,
Assistant Professor, Department of Psychiatry and Neuroscience
University of California, Riverside, CA
MedicalResearch.com: What is the background for this study?
Response: This trial evaluated the effects of pimavanserin compared to placebo in frail older adults and elderly patients with neuropsychiatric symptoms related to Neurodegenerative disorder (NDD), such as hallucinations and delusions, to better understand the safety of pimavanserin in this population.
The study was a phase 3b, 8-week treatment (study duration of up to 16 weeks) with the primary endpoint being safety and tolerability, measured by treatment-emergent adverse events (TEAEs). Secondary safety endpoints were change from baseline in motor and cognitive function; exploratory endpoints included suicidality, sleep quality, and neuropsychiatric symptoms.
The reason for doing this study is that there is a high degree of interest in further understanding the safety of pimavanserin, as many antipsychotics used off label often have significant and serious adverse effects, including risk of falls, parkinsonism, and death.
Dr. Gus Alva[/caption]
Gus Alva, MD, DFAPA
Medical Director, ATP Clinical Research
Medical Director, Senior Brain Health, Hoag Hospital, Newport Beach,
Assistant Professor, Department of Psychiatry and Neuroscience
University of California, Riverside, CA
MedicalResearch.com: What is the background for this study?
Response: This trial evaluated the effects of pimavanserin compared to placebo in frail older adults and elderly patients with neuropsychiatric symptoms related to Neurodegenerative disorder (NDD), such as hallucinations and delusions, to better understand the safety of pimavanserin in this population.
The study was a phase 3b, 8-week treatment (study duration of up to 16 weeks) with the primary endpoint being safety and tolerability, measured by treatment-emergent adverse events (TEAEs). Secondary safety endpoints were change from baseline in motor and cognitive function; exploratory endpoints included suicidality, sleep quality, and neuropsychiatric symptoms.
The reason for doing this study is that there is a high degree of interest in further understanding the safety of pimavanserin, as many antipsychotics used off label often have significant and serious adverse effects, including risk of falls, parkinsonism, and death.
 Dr. Espay[/caption]
Alberto J. Espay, MD, MSc, FAAN
Professor of Neurology
Director and Endowed Chair
Gardner Family Center for Parkinson's disease and Movement Disorders
University of Cincinnati Academic Health Center
MedicalResearch.com: What is the background for this study?
Response: This study was meant to address the gap that current oral levodopa formulations do not suffice to lessen motor fluctuations in people with Parkinson’s disease. IPX203 is a unique extended-release formulation of levodopa.
Dr. Espay[/caption]
Alberto J. Espay, MD, MSc, FAAN
Professor of Neurology
Director and Endowed Chair
Gardner Family Center for Parkinson's disease and Movement Disorders
University of Cincinnati Academic Health Center
MedicalResearch.com: What is the background for this study?
Response: This study was meant to address the gap that current oral levodopa formulations do not suffice to lessen motor fluctuations in people with Parkinson’s disease. IPX203 is a unique extended-release formulation of levodopa.
 Dr. Sun[/caption]
Jiangwei Sun PhD
Postdoctoral researcher
in Prof. Jonas Ludvigsson's group
Department of Medical Epidemiology and Biostatistics
Karolinska Institutet
MedicalResearch.com: What is the background for this study?
Response: A potential infectious etiology has been hypothesized for neurodegenerative diseases, as findings in animal studies have demonstrated that infectious processes might impact pathogenesis, phenotype, and progression of neurodegenerative disease.
The extrapolation of such findings to a human context is however not straightforward. previous studies have mostly examined the role of specific pathogens on a specific neurodegenerative disease, e.g., herpesvirus for Alzheimer’s disease, and influenza, hepatitis C virus, and Helicobacter pylori for PD, with inconclusive results. Although several studies have also assessed associations between infectious diseases and risk of dementia and AD, influence of potential surveillance bias (greater-than-expected surveillance of disease after infections) and reverse causation (due to for example diagnostic delay of neurodegenerative diseases) on the associations was not always fully addressed.
Therefore, whether infection is indeed a risk factor rather a comorbidity or secondary event of neurodegenerative disease remains unknown. In contrast to Alzheimer’s disease, and Parkinson’s disease, the potential link between infection and ALS has been less explored.
Dr. Sun[/caption]
Jiangwei Sun PhD
Postdoctoral researcher
in Prof. Jonas Ludvigsson's group
Department of Medical Epidemiology and Biostatistics
Karolinska Institutet
MedicalResearch.com: What is the background for this study?
Response: A potential infectious etiology has been hypothesized for neurodegenerative diseases, as findings in animal studies have demonstrated that infectious processes might impact pathogenesis, phenotype, and progression of neurodegenerative disease.
The extrapolation of such findings to a human context is however not straightforward. previous studies have mostly examined the role of specific pathogens on a specific neurodegenerative disease, e.g., herpesvirus for Alzheimer’s disease, and influenza, hepatitis C virus, and Helicobacter pylori for PD, with inconclusive results. Although several studies have also assessed associations between infectious diseases and risk of dementia and AD, influence of potential surveillance bias (greater-than-expected surveillance of disease after infections) and reverse causation (due to for example diagnostic delay of neurodegenerative diseases) on the associations was not always fully addressed.
Therefore, whether infection is indeed a risk factor rather a comorbidity or secondary event of neurodegenerative disease remains unknown. In contrast to Alzheimer’s disease, and Parkinson’s disease, the potential link between infection and ALS has been less explored.
 Dr. Khurana[/caption]
Vikram Khurana, MD, PhD
Chief of the Division of Movement Disorders
Department of Neurology
Brigham and Harvard Medical School
Principal investigator, Ann Romney Center for Neurologic Diseases at the Brigham
MedicalResearch.com: What is the background for this study?
Response: Proteins abnormally accumulate in brain cells (neurons and glial cells) in all neurodegenerative diseases. In Parkinson’s disease and related disorders, the key protein that accumulates and aggregates is called “alpha-synuclein.” Presumably, when a protein like alpha-synuclein abnormally folds and aggregates, the abnormal form of the protein can become toxic to the neuron, eventually leading to cell death. Equally, the protein may no longer be able to carry out its normal function.
This begs the question – what does alpha synuclein actually do? Most evidence to date points to alpha-synuclein being involved in the transport of other proteins and chemicals around the cell, by closely associating with vesicles that are small circular containers enclosed by fat (“lipid) membranes. But alpha-synuclein is not just found associated with these vesicle membrane. It is found away from the membrane and it’s been unclear what it does there.
Dr. Khurana[/caption]
Vikram Khurana, MD, PhD
Chief of the Division of Movement Disorders
Department of Neurology
Brigham and Harvard Medical School
Principal investigator, Ann Romney Center for Neurologic Diseases at the Brigham
MedicalResearch.com: What is the background for this study?
Response: Proteins abnormally accumulate in brain cells (neurons and glial cells) in all neurodegenerative diseases. In Parkinson’s disease and related disorders, the key protein that accumulates and aggregates is called “alpha-synuclein.” Presumably, when a protein like alpha-synuclein abnormally folds and aggregates, the abnormal form of the protein can become toxic to the neuron, eventually leading to cell death. Equally, the protein may no longer be able to carry out its normal function.
This begs the question – what does alpha synuclein actually do? Most evidence to date points to alpha-synuclein being involved in the transport of other proteins and chemicals around the cell, by closely associating with vesicles that are small circular containers enclosed by fat (“lipid) membranes. But alpha-synuclein is not just found associated with these vesicle membrane. It is found away from the membrane and it’s been unclear what it does there.
 Clemens R. Scherzer, M.D.
Center for Advanced Parkinson Research
Harvard Medical School
Brigham and Women’s Hospital
Boston, MA
MedicalResearch.com: What is the background for this study?
Response: Parkinson's disease is the fastest growing brain disorder. The number of patients is projected to double to 14 million by 2040. The total cost of Parkinson's is $52 billion every year in the U.S. Yet, there are no medicines available to slow the disease. Current treatments temporarily alleviate symptoms, but do not address the underlying disease process, which continues to relentlessly progress.
To begin to solve this puzzle, we searched the genome of 3,821 Parkinson's disease patients for genetic variants linked to rapid progression over time to dementia, which is a major determinant for a Parkinson's disease patient’s quality of life. These patients were deeply characterized in the International Genetics of Parkinson Disease Progression (IGPP) Consortium, a grass-roots, collaborative network of Parkinson’s investigators, with 31,578 longitudinal study visits over up to 12 years from disease onset.
Clemens R. Scherzer, M.D.
Center for Advanced Parkinson Research
Harvard Medical School
Brigham and Women’s Hospital
Boston, MA
MedicalResearch.com: What is the background for this study?
Response: Parkinson's disease is the fastest growing brain disorder. The number of patients is projected to double to 14 million by 2040. The total cost of Parkinson's is $52 billion every year in the U.S. Yet, there are no medicines available to slow the disease. Current treatments temporarily alleviate symptoms, but do not address the underlying disease process, which continues to relentlessly progress.
To begin to solve this puzzle, we searched the genome of 3,821 Parkinson's disease patients for genetic variants linked to rapid progression over time to dementia, which is a major determinant for a Parkinson's disease patient’s quality of life. These patients were deeply characterized in the International Genetics of Parkinson Disease Progression (IGPP) Consortium, a grass-roots, collaborative network of Parkinson’s investigators, with 31,578 longitudinal study visits over up to 12 years from disease onset.
 Dr. Wenquan Zou[/caption]
Wenquan Zou, MD/PhD, Professor
Department of Pathology
Associate Director
National Prion Disease Pathology Surveillance Center
Case Western Reserve University School of Medicine
Cleveland, Ohio 44106
MedicalResearch.com: What is the background for this study?
Response: Parkinson’s disease (PD) is the second most common age-related neurodegenerative disorder. It is characterized by the accumulation of pathologically misfolded α-synuclein (αSynP) aggregates in the brain. Currently, a definite diagnosis relies on the detection of αSynP-containing Lewy bodies in the brain of PD patients. Development of a reliable and sensitive assay for αSynP in easily accessible peripheral tissue specimens is critical for early or differential diagnosis, determination of disease severity, and evaluation of therapeutic efficacy in clinical trials. Previous studies have revealed that the pathologically phosphorylated α-synuclein is detectable with traditional immunohistochemistry (IHC) and immunofluorescence (IF) microscopy but the sensitivity with IHC/IF is highly variable and inconsistent.
Also the prion-like aggregation seeding activity of αSynP is detected in cerebrospinal fluid (CSF) of Parkinson’s disease patients with highly sensitive real-time quaking-induced conversion (RT-QuIC) and protein misfolding cyclic amplification assays (PMCA). But the lumbar puncture to collect CSF is more invasive compared to skin punch biopsy.
Dr. Wenquan Zou[/caption]
Wenquan Zou, MD/PhD, Professor
Department of Pathology
Associate Director
National Prion Disease Pathology Surveillance Center
Case Western Reserve University School of Medicine
Cleveland, Ohio 44106
MedicalResearch.com: What is the background for this study?
Response: Parkinson’s disease (PD) is the second most common age-related neurodegenerative disorder. It is characterized by the accumulation of pathologically misfolded α-synuclein (αSynP) aggregates in the brain. Currently, a definite diagnosis relies on the detection of αSynP-containing Lewy bodies in the brain of PD patients. Development of a reliable and sensitive assay for αSynP in easily accessible peripheral tissue specimens is critical for early or differential diagnosis, determination of disease severity, and evaluation of therapeutic efficacy in clinical trials. Previous studies have revealed that the pathologically phosphorylated α-synuclein is detectable with traditional immunohistochemistry (IHC) and immunofluorescence (IF) microscopy but the sensitivity with IHC/IF is highly variable and inconsistent.
Also the prion-like aggregation seeding activity of αSynP is detected in cerebrospinal fluid (CSF) of Parkinson’s disease patients with highly sensitive real-time quaking-induced conversion (RT-QuIC) and protein misfolding cyclic amplification assays (PMCA). But the lumbar puncture to collect CSF is more invasive compared to skin punch biopsy.

 Dr. Factor[/caption]
Stewart A. Factor, D.O.
Professor of Neurology
Director of the Movement Disorders Program
Vance Lanier Chair of Neurology
Emory University School of Medicine
MedicalResearch.com: What is the background for this study? Would you briefly explain what is meant by OFF episodes.
Response: Parkinson’s disease (PD) is a chronic, progressive neurodegenerative disease characterized by motor symptoms, including tremor at rest, rigidity and impaired movement, as well as significant non-motor symptoms, such as cognitive impairment, psychiatric symptoms and autonomic symptoms (i.e. urinary issues, constipation, low blood pressure). It is the second-most common neurodegenerative disease after Alzheimer’s disease and it is predicted that the prevalence of Parkinson’s disease will double by the year 2040. The symptoms of PD are in substantial part, due to loss of dopamine nerve cells in the brain. The current standard of care for PD includes replacing the dopamine loss by the use of oral carbidopa/levodopa. Levodopa is a precursor of dopamine, converted in the brain.
OFF episodes have been a significant unmet need in Parkinson’s disease since the emergence of levodopa. Initially, levodopa controls PD symptoms in a continuous fashion throughout the day. With time the response becomes less predictable and patients experience a re-emergence or worsening of PD symptoms. These episodes are what we mean by OFF episodes. OFF episodes can be characterized, in part, by re-emergence of motor symptoms including tremor, stiffness or slowed movement that can happen at any point during the day. OFF episodes typically begin within the first five years of treatment and occur at the end of a dose. This is referred to as end of dose failure or wearing off. Within the first four to six years after diagnosis, regardless of disease severity, up to 60 percent of people with PD experience OFF episodes. With time these episodes become longer, more severe and disabling, more frequent and less predictable as PD progresses. They can take up more than half the day
OFF episodes may alter a persons’ ability to perform everyday activities by slowing or even precluding their completion. The result is significant burden and distress for people living with Parkinson’s disease (PD) and their care partners.
CTH-300 was a Phase 3, 12-week, randomized, double-blind, placebo-controlled, parallel group, study examining the efficacy, safety and tolerability of apomorphine hydrochloride sublingual film (KYNMOBI) in people with levodopa-responsive PD complicated by OFF episodes. The primary endpoint was a mean change in the score from pre-dose in the Movement Disorder Society Unified Parkinson's Disease Rating Scale (MDS-UPDRS) Part III Motor Examination at 30 minutes after dosing at the 12-week visit of the maintenance treatment phase. The key secondary endpoint was the percentage of people with PD with a patient-rated full ON (or best) response within 30 minutes at the 12-week visit of the maintenance treatment phase.
Dr. Factor[/caption]
Stewart A. Factor, D.O.
Professor of Neurology
Director of the Movement Disorders Program
Vance Lanier Chair of Neurology
Emory University School of Medicine
MedicalResearch.com: What is the background for this study? Would you briefly explain what is meant by OFF episodes.
Response: Parkinson’s disease (PD) is a chronic, progressive neurodegenerative disease characterized by motor symptoms, including tremor at rest, rigidity and impaired movement, as well as significant non-motor symptoms, such as cognitive impairment, psychiatric symptoms and autonomic symptoms (i.e. urinary issues, constipation, low blood pressure). It is the second-most common neurodegenerative disease after Alzheimer’s disease and it is predicted that the prevalence of Parkinson’s disease will double by the year 2040. The symptoms of PD are in substantial part, due to loss of dopamine nerve cells in the brain. The current standard of care for PD includes replacing the dopamine loss by the use of oral carbidopa/levodopa. Levodopa is a precursor of dopamine, converted in the brain.
OFF episodes have been a significant unmet need in Parkinson’s disease since the emergence of levodopa. Initially, levodopa controls PD symptoms in a continuous fashion throughout the day. With time the response becomes less predictable and patients experience a re-emergence or worsening of PD symptoms. These episodes are what we mean by OFF episodes. OFF episodes can be characterized, in part, by re-emergence of motor symptoms including tremor, stiffness or slowed movement that can happen at any point during the day. OFF episodes typically begin within the first five years of treatment and occur at the end of a dose. This is referred to as end of dose failure or wearing off. Within the first four to six years after diagnosis, regardless of disease severity, up to 60 percent of people with PD experience OFF episodes. With time these episodes become longer, more severe and disabling, more frequent and less predictable as PD progresses. They can take up more than half the day
OFF episodes may alter a persons’ ability to perform everyday activities by slowing or even precluding their completion. The result is significant burden and distress for people living with Parkinson’s disease (PD) and their care partners.
CTH-300 was a Phase 3, 12-week, randomized, double-blind, placebo-controlled, parallel group, study examining the efficacy, safety and tolerability of apomorphine hydrochloride sublingual film (KYNMOBI) in people with levodopa-responsive PD complicated by OFF episodes. The primary endpoint was a mean change in the score from pre-dose in the Movement Disorder Society Unified Parkinson's Disease Rating Scale (MDS-UPDRS) Part III Motor Examination at 30 minutes after dosing at the 12-week visit of the maintenance treatment phase. The key secondary endpoint was the percentage of people with PD with a patient-rated full ON (or best) response within 30 minutes at the 12-week visit of the maintenance treatment phase.
 Dr. Labrie[/caption]
Dr. Viviane Labrie, PhD
Dr. Labrie is an associate professor in Van Andel Institute’s Center for Neurodegenerative Science, where she studies Parkinson’s, Alzheimer’s and other neurological diseases.
MedicalResearch.com: What is the background for this study?
Response: One of the most puzzling and persistent mysteries in neuroscience has been why some people are “right-brained” while others are “left-brained.” The two sides of the brain have different jobs. The left side is analytic and problem-solving, while the right side manages creativity and artistic talents. But despite their differences, the two sides are composed of the same cell types — essentially, brain neurons and their support cells. In this study, we sought to understand how it is possible for these cells to behave completely differently depending on what hemisphere they’re located in.
We also wanted to examine the reasons behind asymmetry in Parkinson’s disease; that is, why Parkinson’s symptoms typically start on one side of the body before the other. This asymmetry in neurodegeneration and symptoms in patients is one of the biggest unsolved puzzles in the Parkinson’s disease field — why do brain cells in one hemisphere begin dying before brain cells in the other hemisphere?
Dr. Labrie[/caption]
Dr. Viviane Labrie, PhD
Dr. Labrie is an associate professor in Van Andel Institute’s Center for Neurodegenerative Science, where she studies Parkinson’s, Alzheimer’s and other neurological diseases.
MedicalResearch.com: What is the background for this study?
Response: One of the most puzzling and persistent mysteries in neuroscience has been why some people are “right-brained” while others are “left-brained.” The two sides of the brain have different jobs. The left side is analytic and problem-solving, while the right side manages creativity and artistic talents. But despite their differences, the two sides are composed of the same cell types — essentially, brain neurons and their support cells. In this study, we sought to understand how it is possible for these cells to behave completely differently depending on what hemisphere they’re located in.
We also wanted to examine the reasons behind asymmetry in Parkinson’s disease; that is, why Parkinson’s symptoms typically start on one side of the body before the other. This asymmetry in neurodegeneration and symptoms in patients is one of the biggest unsolved puzzles in the Parkinson’s disease field — why do brain cells in one hemisphere begin dying before brain cells in the other hemisphere?

 Donald Weaver, PhD, MD, FRCPC, FCAHS
Senior Scientist and Director, Research Institute
Krembil Research Institute
University Health Network
Toronto, Canada
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: First, we are seeking novel molecules that might have usefulness in the treatment of Alzheimer’s disease (AD). Since Mother Nature is a superb chemist, natural products are an ideal place to start looking for possible therapeutics. There is a long history (penicillin, digitalis …) of drugs identified from natural product sources. Moreover, in earlier work by us, we have shown that other natural products extracted from maple syrup have possible therapeutic efficacy against AD.
Therefore, it was logical for us to look at extracts of coffee. We see similarities between maple syrup and coffee. In both of these natural products, the plant derived material (i.e. the coffee bean, or sap from maple syrup) is initially boiled or roasted prior to its use; thus, it is not a direct simple plant product, but one that has been heated (boiled or roasted). We suspect that the heating process “does more chemistry” enabling the generation of new molecules from the plant derived materials. In our study we show that a class of compounds (phenylindanes) from roasted coffee has the ability to inhibit the misfolding of two proteins (beta-amyloid, tau) whose misfolding and aggregation (“clumping”) is implicated in the disease process of AD.
Second, as described below, there is already epidemiological evidence that coffee consumption may offer some protective effects against Alzheimer’s disease and Parkinson’s disease (PD), so by looking at the constituents of coffee for chemicals that might block the clumping of beta-amyloid and/or tau, was an attempt to seek a molecular link explaining the epidemiology.
Donald Weaver, PhD, MD, FRCPC, FCAHS
Senior Scientist and Director, Research Institute
Krembil Research Institute
University Health Network
Toronto, Canada
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: First, we are seeking novel molecules that might have usefulness in the treatment of Alzheimer’s disease (AD). Since Mother Nature is a superb chemist, natural products are an ideal place to start looking for possible therapeutics. There is a long history (penicillin, digitalis …) of drugs identified from natural product sources. Moreover, in earlier work by us, we have shown that other natural products extracted from maple syrup have possible therapeutic efficacy against AD.
Therefore, it was logical for us to look at extracts of coffee. We see similarities between maple syrup and coffee. In both of these natural products, the plant derived material (i.e. the coffee bean, or sap from maple syrup) is initially boiled or roasted prior to its use; thus, it is not a direct simple plant product, but one that has been heated (boiled or roasted). We suspect that the heating process “does more chemistry” enabling the generation of new molecules from the plant derived materials. In our study we show that a class of compounds (phenylindanes) from roasted coffee has the ability to inhibit the misfolding of two proteins (beta-amyloid, tau) whose misfolding and aggregation (“clumping”) is implicated in the disease process of AD.
Second, as described below, there is already epidemiological evidence that coffee consumption may offer some protective effects against Alzheimer’s disease and Parkinson’s disease (PD), so by looking at the constituents of coffee for chemicals that might block the clumping of beta-amyloid and/or tau, was an attempt to seek a molecular link explaining the epidemiology.
 Dr. Labrie[/caption]
Viviane Labrie, Ph.D.
Assistant Professor
Center for Neurodegenerative Science
Van Andel Research Institute
Grand Rapids, Michigan
MedicalResearch.com: What is the background for this study?
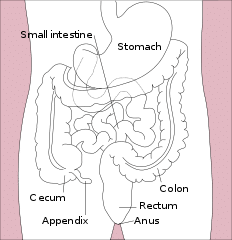
Response: Our lab has an interest in the early events and initiation of neurodegenerative diseases. Parkinson’s disease for a long time was thought to be a movement disorder driven by the destruction of dopamine neurons in a specific area of the brain, the substantia nigra. In the last 10 years it has become evident that Parkinson’s disease is not just a movement disorder but hosts a whole range of non-motor systems. One of the most common non-motor symptoms in Parkinson’s patients is issues with the gastrointestinal (GI) tract. GI symptoms often occur early in Parkinson’s disease; for many patients, GI symptoms precede the onset of motor symptoms by as many as 2 decades. Moreover, the GI is not only involved in the early signs of Parkinson’s but has been proposed to be a place in the body where Parkinson’s disease begins.
The hallmark pathology of Parkinson’s disease in the brain is Lewy bodies, which contains a clumped form of a protein called alpha-synuclein. There is evidence that Parkinson’s disease pathology, this clumped alpha-synuclein protein, is detectable in the GI tract, even many years before the onset of Parkinson’s motor symptoms. Clumped alpha-synuclein is also capable of traveling across nerve cells. There is evidence that clumped alpha-synuclein can travel up the nerve that connects the GI tract to the brain and enter the brain. This could be disastrous because clumped alpha-synuclein can seed and spread in the brain, which has neurotoxic effects and can eventually lead to Parkinson’s disease. In fact, in the brain of Parkinson’s patients, one of the first places where alpha-synuclein clumps are detected is at the terminal where the gut nerve connects to the brain, and this pathology advances from this point to other brain areas as the disease progresses.
This intriguing connection of the GI tract to the early processes of Parkinson’s disease had us interested in trying to understand how the gut could be involved in triggering Parkinson’s. But the GI tract is a very big place, and we first asked ourselves, where should we look to better understand GI involvement in Parkinson’s disease?
Dr. Labrie[/caption]
Viviane Labrie, Ph.D.
Assistant Professor
Center for Neurodegenerative Science
Van Andel Research Institute
Grand Rapids, Michigan
MedicalResearch.com: What is the background for this study?
Response: Our lab has an interest in the early events and initiation of neurodegenerative diseases. Parkinson’s disease for a long time was thought to be a movement disorder driven by the destruction of dopamine neurons in a specific area of the brain, the substantia nigra. In the last 10 years it has become evident that Parkinson’s disease is not just a movement disorder but hosts a whole range of non-motor systems. One of the most common non-motor symptoms in Parkinson’s patients is issues with the gastrointestinal (GI) tract. GI symptoms often occur early in Parkinson’s disease; for many patients, GI symptoms precede the onset of motor symptoms by as many as 2 decades. Moreover, the GI is not only involved in the early signs of Parkinson’s but has been proposed to be a place in the body where Parkinson’s disease begins.
The hallmark pathology of Parkinson’s disease in the brain is Lewy bodies, which contains a clumped form of a protein called alpha-synuclein. There is evidence that Parkinson’s disease pathology, this clumped alpha-synuclein protein, is detectable in the GI tract, even many years before the onset of Parkinson’s motor symptoms. Clumped alpha-synuclein is also capable of traveling across nerve cells. There is evidence that clumped alpha-synuclein can travel up the nerve that connects the GI tract to the brain and enter the brain. This could be disastrous because clumped alpha-synuclein can seed and spread in the brain, which has neurotoxic effects and can eventually lead to Parkinson’s disease. In fact, in the brain of Parkinson’s patients, one of the first places where alpha-synuclein clumps are detected is at the terminal where the gut nerve connects to the brain, and this pathology advances from this point to other brain areas as the disease progresses.
This intriguing connection of the GI tract to the early processes of Parkinson’s disease had us interested in trying to understand how the gut could be involved in triggering Parkinson’s. But the GI tract is a very big place, and we first asked ourselves, where should we look to better understand GI involvement in Parkinson’s disease?

 Dr. Willis[/caption]
Allison W. Willis, MD, MS
Assistant Professor of Neurology
Assistant Professor of Biostatistics and Epidemiology
Senior Fellow, Leonard Davis Institute
Senior Scholar, Center for Clinical Epidemiology and Biostatistics
University of Pennsylvania School of Medicine
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: This study was motivated by my own experiences as a neurologist-neuroscientist.
I care for Parkinson disease patients, and over the year, have had numerous instances in which a person was taking a medication that could interact with their Parkinson disease medications, or could worsen their PD symptoms.
Dr. Willis[/caption]
Allison W. Willis, MD, MS
Assistant Professor of Neurology
Assistant Professor of Biostatistics and Epidemiology
Senior Fellow, Leonard Davis Institute
Senior Scholar, Center for Clinical Epidemiology and Biostatistics
University of Pennsylvania School of Medicine
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: This study was motivated by my own experiences as a neurologist-neuroscientist.
I care for Parkinson disease patients, and over the year, have had numerous instances in which a person was taking a medication that could interact with their Parkinson disease medications, or could worsen their PD symptoms.

 Fudi Wang, M.D., Ph.D.
Qiushi Chair Professor
Nutrition Discovery Innovation Center
School of Public Health/School of Medicine
Zhejiang University
Hangzhou China
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Parkinson disease (PD) is the second most common neurodegenerative disease affecting approximately 10 million people around the world. To date, the cause of PD remains poorly understood. It is reported that 90% PD cases have no identifiable genetic cause. What’s worse, few therapeutic advances for the treatment of PD have been made in the past decades. Nevertheless, growing prospective longitudinal studies shed lights on the potential beneficial effect of lifestyle factors on reducing the risk of developing Parkinson disease. In this study, we performed a a dose-response meta-analysis of more than half a million participants.
We found that physical activity, particularly moderate to vigorous physical activity, could significantly reduce PD risk.
Fudi Wang, M.D., Ph.D.
Qiushi Chair Professor
Nutrition Discovery Innovation Center
School of Public Health/School of Medicine
Zhejiang University
Hangzhou China
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Parkinson disease (PD) is the second most common neurodegenerative disease affecting approximately 10 million people around the world. To date, the cause of PD remains poorly understood. It is reported that 90% PD cases have no identifiable genetic cause. What’s worse, few therapeutic advances for the treatment of PD have been made in the past decades. Nevertheless, growing prospective longitudinal studies shed lights on the potential beneficial effect of lifestyle factors on reducing the risk of developing Parkinson disease. In this study, we performed a a dose-response meta-analysis of more than half a million participants.
We found that physical activity, particularly moderate to vigorous physical activity, could significantly reduce PD risk.

Joseph Jankovic, MD Professor of Neurology Distinguished Chair in Movement Disorders Director, Parkinson’s Disease Center and Movement Disorders Clinic Department of Neurology Baylor College of Medicine Baylor St. Luke’s Medical Center at the McNair Campus Houston, TX 77030-4202 MedicalResearch.com: What should readers take away from your study? First demonstration of an anti-α-synuclein antibody immunotherapy in patients with Parkinson’s Disease. Robust target...
 Benjamin Dawson[/caption]
Benjamin Dawson, B.Sc.
MD Candidate 2020
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Dementia in Parkinson’s Disease is one of its most feared complications, and may happen eventually to most patients if they reached advanced age. Identifying those at especially high risk of dementia has important potential implications - it would facilitate clinical counselling, it has treatment implications (e.g. knowing a person is likely to get dementia in the near future would probably steer you away from certain medications and towards others). Most critically, it can help select patients for trials to prevent dementia.
While several factors that show high risk for dementia in Parkinson’s disease have previously been described, these have yet to shape patient-care, either because they are not very strong predictors, or they are not user-friendly. So, we designed a very simple clinical screening tool, called the Montreal Parkinson’s Risk of Dementia Scale (MoPaRDS). It took predictors of dementia that were established from large-scale studies and boiled them down into a simple 8-point scale that uses information that you can get in a simple office visit. The 8 predictors were being over 70, being male, having a blood pressure drop with standing, showing early mild cognitive changes, having a symmetric bilateral disease (that is, one side not clearly worse than the other), experiencing falls or freezing, having experienced hallucinations, and having symptoms of REM sleep behavior disorder ('acting out' the dreams at night).
When we tested the scale in a combined cohort of 607 patients with Parkinson’s (of whom 70 developed dementia over mean follow-up of 4.4-years) a positive MoPaRDS screen (≥4 out of 8 items) identified 14-fold increased risk of dementia compared to a negative screen. We recommend dividing the scale into three categories; low-, intermediate- and high-risk. Those in the highest score group (MoPaRDS, 6-8) had a 14.9% risk of developing dementia each year, while those with the lowest scores (MoPaRDS, 0-3) had only 0.6% annual risk. So, these simple measures can be pretty powerful predictors of dementia.
Benjamin Dawson[/caption]
Benjamin Dawson, B.Sc.
MD Candidate 2020
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Dementia in Parkinson’s Disease is one of its most feared complications, and may happen eventually to most patients if they reached advanced age. Identifying those at especially high risk of dementia has important potential implications - it would facilitate clinical counselling, it has treatment implications (e.g. knowing a person is likely to get dementia in the near future would probably steer you away from certain medications and towards others). Most critically, it can help select patients for trials to prevent dementia.
While several factors that show high risk for dementia in Parkinson’s disease have previously been described, these have yet to shape patient-care, either because they are not very strong predictors, or they are not user-friendly. So, we designed a very simple clinical screening tool, called the Montreal Parkinson’s Risk of Dementia Scale (MoPaRDS). It took predictors of dementia that were established from large-scale studies and boiled them down into a simple 8-point scale that uses information that you can get in a simple office visit. The 8 predictors were being over 70, being male, having a blood pressure drop with standing, showing early mild cognitive changes, having a symmetric bilateral disease (that is, one side not clearly worse than the other), experiencing falls or freezing, having experienced hallucinations, and having symptoms of REM sleep behavior disorder ('acting out' the dreams at night).
When we tested the scale in a combined cohort of 607 patients with Parkinson’s (of whom 70 developed dementia over mean follow-up of 4.4-years) a positive MoPaRDS screen (≥4 out of 8 items) identified 14-fold increased risk of dementia compared to a negative screen. We recommend dividing the scale into three categories; low-, intermediate- and high-risk. Those in the highest score group (MoPaRDS, 6-8) had a 14.9% risk of developing dementia each year, while those with the lowest scores (MoPaRDS, 0-3) had only 0.6% annual risk. So, these simple measures can be pretty powerful predictors of dementia.
 Prof. Hausforff[/caption]
Prof. Jeffrey Hausdorff PhD
Director of the Center for the Study of Movement, Cognition and Mobility
Full Professor in the Sackler School of Medicine and Sagol School of Neuroscience
Tel Aviv Medical Center
MedicalResearch.com: What is the background for this study?
Response: Many people with Parkinson’s disease suffer from a disturbing symptom referred to as “freezing of gait”. When freezing occurs, the person’s feet inexplicably become stuck to the floor and he or she is unable to move forward, despite efforts to walk. Initially, the problem can last just a few seconds and occur very infrequently. As the problem progresses, however, freezing can last many seconds, occurring frequently throughout the day. This can lead to a very frustrating situation that may also be dangerous. People with freezing of gait have an increased risk of falls and reduced health-related quality of life.
The behavioral manifestation of freezing of gait is a problem with walking, i.e., it is a “motor” symptom. However, there is also evidence that deficits in specific aspects of cognitive function (i.e., executive function) may also contribute to freezing of gait. The goals of the present work were to use non-invasive brain stimulation to better understand if these cognitive deficits are indeed in the causal chain and if non-invasive brain stimulation that simultaneously targets both motor and cognitive brain areas that are believed to involved with freezing have a better impact on freezing and related symptoms than stimulation that targets only motor brain areas or sham stimulation.
Prof. Hausforff[/caption]
Prof. Jeffrey Hausdorff PhD
Director of the Center for the Study of Movement, Cognition and Mobility
Full Professor in the Sackler School of Medicine and Sagol School of Neuroscience
Tel Aviv Medical Center
MedicalResearch.com: What is the background for this study?
Response: Many people with Parkinson’s disease suffer from a disturbing symptom referred to as “freezing of gait”. When freezing occurs, the person’s feet inexplicably become stuck to the floor and he or she is unable to move forward, despite efforts to walk. Initially, the problem can last just a few seconds and occur very infrequently. As the problem progresses, however, freezing can last many seconds, occurring frequently throughout the day. This can lead to a very frustrating situation that may also be dangerous. People with freezing of gait have an increased risk of falls and reduced health-related quality of life.
The behavioral manifestation of freezing of gait is a problem with walking, i.e., it is a “motor” symptom. However, there is also evidence that deficits in specific aspects of cognitive function (i.e., executive function) may also contribute to freezing of gait. The goals of the present work were to use non-invasive brain stimulation to better understand if these cognitive deficits are indeed in the causal chain and if non-invasive brain stimulation that simultaneously targets both motor and cognitive brain areas that are believed to involved with freezing have a better impact on freezing and related symptoms than stimulation that targets only motor brain areas or sham stimulation.
 Dr. Saunders-Pullman[/caption]
Rachel Saunders-Pullman, MD, MPH
Associate Professor of Neurology
Icahn School of Medicine at Mount Sinai
Chief, Movement Disorders, Mount Sinai Beth Israel
Co-Director Clinical/Translational Research and Research Mentoring
Movement Disorders, Department of Neurology,
Mount Sinai Beth Israel
New York, NY 10003
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: There is a diversity in causes of Parkinson’s Disease (PD), and this may lead to heterogeneity in drug response. While LRRK2 PD due to G2019S mutations may fully mimic idiopathic PD (IPD), cross-sectional study suggests that the course may be slightly milder than IPD. Further, the pathology is heterogeneous with a minority not demonstrating Lewy bodies, and this may also correspond to less severe non-motor features.
To better understand the course of PD associated with the G2019S LRRK2 mutation (the most common LRRK2 mutation), we evaluated motor and cognitive progression in individuals enrolled in the LRRK2 Ashkenazi Jewish Consortium. Subjects were recruited from a Center in Tel Aviv, Israel, Sourasky Medical Center, and from two centers in New York, Columbia University and Mount Sinai Beth Israel. 144 participants were LRRK2 mutation carriers and 401 were not. We utilized all study visits, and constructed linear mixed-effects models to estimate the association between harboring the LRRK2 mutation and rate of change of both motor features- as assessed by the Unified Parkinson’s Disease Rating Scale (UPDRS), and cognition, as measured by the Montreal Cognitive Assessment Scale (MoCA). Models adjusted for sex, site, age, disease duration and (for the motor models) cognitive score.
We found a small but significant difference in rate of progression, with LRRK2 PD progressing at 0.69 points/year, and IPD at 1.06 points/year. While the cognitive decline was also less in the LRRK2 PD (-0.10 vs. -0.19 in the IPD, this difference was not statistically different (p=0.08).
Dr. Saunders-Pullman[/caption]
Rachel Saunders-Pullman, MD, MPH
Associate Professor of Neurology
Icahn School of Medicine at Mount Sinai
Chief, Movement Disorders, Mount Sinai Beth Israel
Co-Director Clinical/Translational Research and Research Mentoring
Movement Disorders, Department of Neurology,
Mount Sinai Beth Israel
New York, NY 10003
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: There is a diversity in causes of Parkinson’s Disease (PD), and this may lead to heterogeneity in drug response. While LRRK2 PD due to G2019S mutations may fully mimic idiopathic PD (IPD), cross-sectional study suggests that the course may be slightly milder than IPD. Further, the pathology is heterogeneous with a minority not demonstrating Lewy bodies, and this may also correspond to less severe non-motor features.
To better understand the course of PD associated with the G2019S LRRK2 mutation (the most common LRRK2 mutation), we evaluated motor and cognitive progression in individuals enrolled in the LRRK2 Ashkenazi Jewish Consortium. Subjects were recruited from a Center in Tel Aviv, Israel, Sourasky Medical Center, and from two centers in New York, Columbia University and Mount Sinai Beth Israel. 144 participants were LRRK2 mutation carriers and 401 were not. We utilized all study visits, and constructed linear mixed-effects models to estimate the association between harboring the LRRK2 mutation and rate of change of both motor features- as assessed by the Unified Parkinson’s Disease Rating Scale (UPDRS), and cognition, as measured by the Montreal Cognitive Assessment Scale (MoCA). Models adjusted for sex, site, age, disease duration and (for the motor models) cognitive score.
We found a small but significant difference in rate of progression, with LRRK2 PD progressing at 0.69 points/year, and IPD at 1.06 points/year. While the cognitive decline was also less in the LRRK2 PD (-0.10 vs. -0.19 in the IPD, this difference was not statistically different (p=0.08).
 Dr. Mehellou[/caption]
Dr. Youcef Mehellou PhD
Lecturer in Medicinal Chemistry
Cardiff School of Pharmacy and Pharmaceutical Sciences
Cardiff University
MedicalResearch.com: What is the background for this study?
Response: Over the last decade or two, there has been many reports linking genetic mutations to the pathogenesis of Parkinson’s disease (PD). Among the proteins that have been found to be mutated in PD is a protein called PINK1. Indeed, PINK1 mutations that disturb its function in cells were found to be causal of PD in humans. Subsequent studies showed that PINK1 is a major player in maintaining healthy neurons. This is because it is one of the components involved in controlling the quality of the mitochondria, an organelle within the cell, and it does this by triggering the disposal of unhealthy mitochondria. Overall, studies into PINK1 indicated that the activation of PINK1 as a plausible strategy for maintaining health neurons and hence slowing down the development and progress of Parkinson’s disease.
Dr. Mehellou[/caption]
Dr. Youcef Mehellou PhD
Lecturer in Medicinal Chemistry
Cardiff School of Pharmacy and Pharmaceutical Sciences
Cardiff University
MedicalResearch.com: What is the background for this study?
Response: Over the last decade or two, there has been many reports linking genetic mutations to the pathogenesis of Parkinson’s disease (PD). Among the proteins that have been found to be mutated in PD is a protein called PINK1. Indeed, PINK1 mutations that disturb its function in cells were found to be causal of PD in humans. Subsequent studies showed that PINK1 is a major player in maintaining healthy neurons. This is because it is one of the components involved in controlling the quality of the mitochondria, an organelle within the cell, and it does this by triggering the disposal of unhealthy mitochondria. Overall, studies into PINK1 indicated that the activation of PINK1 as a plausible strategy for maintaining health neurons and hence slowing down the development and progress of Parkinson’s disease.
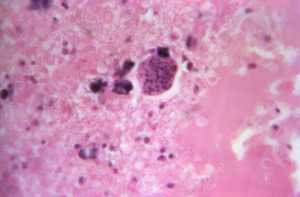 Under a magnification of 900X, this hematoxylin and eosin-stained (H&E) photomicrograph of a brain tissue specimen revealed a case of neurotoxoplasmosis in a patient who had also been diagnosed with multiple myeloma. Note the Toxoplasma gondii tissue cyst, within which bradyzoites could be seen developing. CDC Image[/caption]
Rima McLeod, M.D., F.A.C.P, F.I.D.S.A
Professor of Ophthalmology and Visual Sciences,Pediatrics (Infectious Diseases), and The College,
Director, Toxoplasmosis Center,
Senior Fellow,Institute of Genomics, Genetics and Systems Biology, Member, Commitees on Immunology, and Molecular Medicine and Pathogenesis,
Member Global Health Center, Affiliate CHeSS;
Attending Physician, Chicago Medicine,
The University of Chicago
MedicalResearch.com: What is the background for this study?
* One third of humans are infected lifelong with the brain-dwelling, protozoan parasite, Toxoplasma gondii.
* Approximately fifteen million of these have congenital toxoplasmosis.
* The parasite interconverts between slow-growing, encysted bradyzoites and rapid-growing tachyzoites.
* In mice, T. gondii creates a chronic intra-neuronal infection and an inflammatory process.
* Mice with acute and chronic infection have alterations in neurotransmitters, memory, seizures, and neurobehavior.
* Some epidemiologic-serologic studies show associations between seropositivity for T. gondii and human neurologic diseases, for example, Parkinson’s and Alzheimer’s diseases.
* Although neurobehavioral disease is associated with seropositivity, causality is unproven.
* Serologic studies of humans with diverse genetics are not optimal to detect strong associations or directionality.
* Epidemiologic associations also do not reveal parasite-modulated gene networks in human brain that could provide insights into how to cure and prevent resultant diseases.
* We need integrative approaches to examine relationships between brain parasitism and other brain diseases, to provide a foundation to identify key pathways and molecules for drug and vaccine design
* To address these problems, we considered two central questions: (i) If chronic brain parasitism associates with other neurologic diseases, what are they? And (ii) Which macromolecular networks are modulated by the parasite in human brain that lead to neuropathology which could underpin and facilitate design of treatments?
* We hypothesized that a systems approach integrating multiple levels of host parasite interactions might resolve these questions.
* To better understand what this parasite does to human brains, we performed a comprehensive systems analysis of the infected brain.
Under a magnification of 900X, this hematoxylin and eosin-stained (H&E) photomicrograph of a brain tissue specimen revealed a case of neurotoxoplasmosis in a patient who had also been diagnosed with multiple myeloma. Note the Toxoplasma gondii tissue cyst, within which bradyzoites could be seen developing. CDC Image[/caption]
Rima McLeod, M.D., F.A.C.P, F.I.D.S.A
Professor of Ophthalmology and Visual Sciences,Pediatrics (Infectious Diseases), and The College,
Director, Toxoplasmosis Center,
Senior Fellow,Institute of Genomics, Genetics and Systems Biology, Member, Commitees on Immunology, and Molecular Medicine and Pathogenesis,
Member Global Health Center, Affiliate CHeSS;
Attending Physician, Chicago Medicine,
The University of Chicago
MedicalResearch.com: What is the background for this study?
* One third of humans are infected lifelong with the brain-dwelling, protozoan parasite, Toxoplasma gondii.
* Approximately fifteen million of these have congenital toxoplasmosis.
* The parasite interconverts between slow-growing, encysted bradyzoites and rapid-growing tachyzoites.
* In mice, T. gondii creates a chronic intra-neuronal infection and an inflammatory process.
* Mice with acute and chronic infection have alterations in neurotransmitters, memory, seizures, and neurobehavior.
* Some epidemiologic-serologic studies show associations between seropositivity for T. gondii and human neurologic diseases, for example, Parkinson’s and Alzheimer’s diseases.
* Although neurobehavioral disease is associated with seropositivity, causality is unproven.
* Serologic studies of humans with diverse genetics are not optimal to detect strong associations or directionality.
* Epidemiologic associations also do not reveal parasite-modulated gene networks in human brain that could provide insights into how to cure and prevent resultant diseases.
* We need integrative approaches to examine relationships between brain parasitism and other brain diseases, to provide a foundation to identify key pathways and molecules for drug and vaccine design
* To address these problems, we considered two central questions: (i) If chronic brain parasitism associates with other neurologic diseases, what are they? And (ii) Which macromolecular networks are modulated by the parasite in human brain that lead to neuropathology which could underpin and facilitate design of treatments?
* We hypothesized that a systems approach integrating multiple levels of host parasite interactions might resolve these questions.
* To better understand what this parasite does to human brains, we performed a comprehensive systems analysis of the infected brain.
 Dr. Wirdefeldt[/caption]
Karin Wirdefeldt, MD, PhD
Associate professor
Karolinska Institutet
Stockholm, Sweden
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: It has been hypothesized that Parkinson's disease may start in the gut and spread to the brain via the vagal nerve. We found that people who had a truncal vagotomy (ie, the nerve trunk fully resected) at least 5 years earlier were less likely to develop Parkinson's disease compared to people without vagotomy or people who had a selective vagotomy (ie, only branches of the nerve resected).
Dr. Wirdefeldt[/caption]
Karin Wirdefeldt, MD, PhD
Associate professor
Karolinska Institutet
Stockholm, Sweden
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: It has been hypothesized that Parkinson's disease may start in the gut and spread to the brain via the vagal nerve. We found that people who had a truncal vagotomy (ie, the nerve trunk fully resected) at least 5 years earlier were less likely to develop Parkinson's disease compared to people without vagotomy or people who had a selective vagotomy (ie, only branches of the nerve resected).
 Dr. Patrik Brundin[/caption]
Patrik Brundin, M.D., Ph.D.
Director, Center for Neurodegenerative Science
Van Andel Research Institute
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: The investigational drug at the heart of our study, MSDC-0160, has been in development to treat type 2 diabetes by improving cellular metabolism.
In Parkinson’s, reductions in cellular metabolism slow down vital housekeeping processes that clear out toxic proteins that otherwise accumulate with age. If these proteins aren’t removed, they clump together, leading to the damage and cell death that causes Parkinson’s hallmark symptoms, such as rigidity and tremor. MSDC-0160 helps keep these housekeeping processes working, ultimately protecting the brain.
We demonstrated that MSDC-0160 has strong, reproducible, positive effects across multiple models of Parkinson’s disease—it rescued dopamine-producing cells, improved behavioral deficits in mouse models and reversed inflammation. Overall, we believe it is a strong candidate for repurposing as a potential treatment that actually may slow the disease’s progression, rather than only mitigating symptoms.
Dr. Patrik Brundin[/caption]
Patrik Brundin, M.D., Ph.D.
Director, Center for Neurodegenerative Science
Van Andel Research Institute
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: The investigational drug at the heart of our study, MSDC-0160, has been in development to treat type 2 diabetes by improving cellular metabolism.
In Parkinson’s, reductions in cellular metabolism slow down vital housekeeping processes that clear out toxic proteins that otherwise accumulate with age. If these proteins aren’t removed, they clump together, leading to the damage and cell death that causes Parkinson’s hallmark symptoms, such as rigidity and tremor. MSDC-0160 helps keep these housekeeping processes working, ultimately protecting the brain.
We demonstrated that MSDC-0160 has strong, reproducible, positive effects across multiple models of Parkinson’s disease—it rescued dopamine-producing cells, improved behavioral deficits in mouse models and reversed inflammation. Overall, we believe it is a strong candidate for repurposing as a potential treatment that actually may slow the disease’s progression, rather than only mitigating symptoms.
 Dr. Adolfo Ramirez Zamora[/caption]
Adolfo Ramirez Zamora, MD
Associate Professor of Neurology and
Phyllis E. Dake Endowed Chair in Movement Disorders
Department of Neurology
Albany Medical College
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Patients with SPG 11 mutations can present with motor symptoms characterized by juvenile onset dystonia, Parkinsonism and lower extremity spasticity. Parkinsonism appears to be responsive to levodopa therapy early in the disease but treatment is complicated by the occurrence of motor fluctuations resembling parkinson disease. Patients have short duration of medication effects, unpredictable response to medications along with generalized, excessive involuntary movements known as dyskinesias.
Deep Brain stimulation is a well-established treatment for movement disorders but it has never been used in this disease. We first report the clinical outcome obtained with globus pallidus internal deep brain stimulation in a patient with parkinsonism, dystonia, dyskinesias related to SPG 11. Additionally, we report for the first time the basal ganglia changes observed in the disease using intraoperative neuronal recordings. Patient had a sustained and remarkable response to stimulation over the next two years without side effects. Neurophysiologic changes revealed a unique pattern of neuronal firing despite of the resemblance to advance Parkinsons disease.
Dr. Adolfo Ramirez Zamora[/caption]
Adolfo Ramirez Zamora, MD
Associate Professor of Neurology and
Phyllis E. Dake Endowed Chair in Movement Disorders
Department of Neurology
Albany Medical College
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Patients with SPG 11 mutations can present with motor symptoms characterized by juvenile onset dystonia, Parkinsonism and lower extremity spasticity. Parkinsonism appears to be responsive to levodopa therapy early in the disease but treatment is complicated by the occurrence of motor fluctuations resembling parkinson disease. Patients have short duration of medication effects, unpredictable response to medications along with generalized, excessive involuntary movements known as dyskinesias.
Deep Brain stimulation is a well-established treatment for movement disorders but it has never been used in this disease. We first report the clinical outcome obtained with globus pallidus internal deep brain stimulation in a patient with parkinsonism, dystonia, dyskinesias related to SPG 11. Additionally, we report for the first time the basal ganglia changes observed in the disease using intraoperative neuronal recordings. Patient had a sustained and remarkable response to stimulation over the next two years without side effects. Neurophysiologic changes revealed a unique pattern of neuronal firing despite of the resemblance to advance Parkinsons disease.