

18 May ChatCPR: Could AI Save Lives During Out-of-Hospital Cardiac Arrest?
MedicalResearch.com Interview with:
Nimit Desai, BA
Medical Student and Affiliate Researcher
UC San Diego School of Medicine and Qualcomm Institute
John W. Ayers, PhD, MA
Vice Chief of Innovation, Head of AI, and Professor
UC San Diego School of Medicine, Altman Clinic and Translational Research Institute, and Qualcomm Institute
Christopher Horvat, MD, MHA, MSIT
Associate Professor of Critical Care Medicine, Pediatrics, Biomedical Informatics, and Clinical & Translational Science
Associate Director, Safar Center for Resuscitation Research
More than 350,000 Americans go into cardiac arrest outside a hospital every year, yet only about 2% of the population is certified in CPR. When someone collapses, most bystanders call 911 and wait — and even when dispatchers walk callers through CPR instructions, it often takes nearly three minutes before chest compressions begin. Researchers at UC San Diego set out to close that gap with AI.
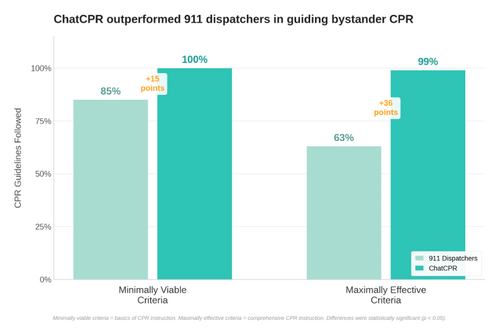
The result is ChatCPR, an open-source AI system built on actual 911 dispatcher training protocols and decades of CPR evidence. In head-to-head comparisons using real, de-identified 911 calls, ChatCPR outperformed human dispatchers on every measure — scoring 15 percentage points higher on basic steps and 36 points higher on advanced steps.
MedicalResearch.com: What is the background for this study?
Response: There are over 178,000 published articles about AI in medicine. But “when will AI actually save lives?” We didn’t have a good answer. So that question became the starting point.
We looked at where AI could make the biggest immediate difference, not in documentation or billing or any of that, but in a moment where seconds literally determine whether someone lives or dies. And the answer was obvious: out-of-hospital cardiac arrest.
More than 350,000 Americans go into cardiac arrest outside a hospital every year. Yet, only about 2% of us are certified in CPR. When someone collapses from an arrest, most people just call 911 and wait, and wait, and wait. And even when dispatchers eventually walk callers through CPR instructions, they’re juggling multiple tasks and it often takes nearly 3 minutes before chest compressions even start. We thought AI could close that gap.
MedicalResearch.com: Would you describe ChatCPR?
Response: ChatCPR is an open-source AI system that we’ve published freely for anyone to use, study, and build on. We deliberately open-sourced everything because this only works if it’s universally accessible.
Think of ChatCPR as a blueprint and a working prototype. We’ve released the complete system, the evaluation framework, everything, so that developers and technology companies can take it and integrate it into the tools people already use like Apple’s Siri, OpenAI’s ChatGPT, or xAI’s Grok.
As for the master vision, imagine you’re with someone who collapses — you could ask Siri, Google Assistant, Alexa, or whatever AI assistant is on your phone, “Help me do CPR,” and immediately get step-by-step, reactive, and guideline-based coaching. Voice activation is absolutely where this needs to go, because in a real emergency you can’t be scrolling through an app. Your hands need to be on the person’s chest.
Expansion of our system because of our open source framework is immediately achievable, such as translation. The underlying AI models already support dozens of languages. A Spanish-speaking version, or any other language, is a natural next step. In fact, that’s one of the advantages over the current system: it takes months to effectively train and then source a 911 dispatcher, but AI can be instantly retrained and deployed at scale with little cost.
MedicalResearch.com: What are the main findings?
Response: We did our study and the development of ChatCPR in two phases. First, we took all the big-name AI models — ChatGPT, Claude, Grok, Gemini, Llama, Mixtral — and tested them on CPR coaching in simulated arrest scenarios. They did okay on the basics, averaging about 90% on essential steps like telling you where to press and how fast. But when it came to the more advanced instructions that really optimize survival, like making sure you let the chest fully rise between compressions, they dropped to around 70%. And in cardiac arrest, 70% isn’t good enough. Missing just 10 or even 30% of steps can be the difference between life and death.
So we built ChatCPR from the ground up, grounded in actual 911 dispatcher training protocols and decades of CPR evidence. It scored 100% on both basic and advanced checklists in simulated scenarios.
Then came the real test. We took actual public, de-identified 911 calls where dispatchers had coached callers through CPR, and we compared what the dispatchers said to what ChatCPR would have said. ChatCPR won every single head-to-head comparison. It performed 15 percentage points better on basic steps and 36 points better on advanced steps. It was especially strong in areas where overwhelmed, multitasking dispatchers tend to falter: patient assessment, compression depth and rate, and chest recoil.
MedicalResearch.com: What should readers take away from your report?
Response: The big takeaway is that AI doesn’t have to be theoretical or futuristic in medicine. This is a concrete example of AI that could help save lives right now, today, if we get it into the right hands. Dispatchers do an incredible job under unbelievable stress. But AI doesn’t get tired, doesn’t forget steps, and delivers the same quality instructions at 3 AM as it does at 3 PM. It can be a tool that makes the whole system better. Yet the implications of our system apply to other scenarios, like coaching health professionals, dispatchers, and lay persons to prepare for assisting with CPR in future emergencies.
The other takeaway is that off-the-shelf AI wasn’t good enough. It took real clinical expertise, emergency medicine knowledge, and careful engineering to build something that actually works. That’s the model for how AI in healthcare should be done — not just throwing a chatbot at a problem, but deeply integrating domain expertise into the system.
MedicalResearch.com: What recommendations do you have for future research?
Response: The obvious next step is real-world testing. We need clinical trials that put ChatCPR in actual emergency situations with real callers, real stress, real chaos and measure whether it actually improves outcomes. Does it get compressions started faster? Does it improve survival? Those are the questions that matter.
We also need usability research. How do panicked people actually interact with an AI coach in the worst moment of their life? Is a voice interface best, or do some people need visual prompts? What happens when there’s background noise, or the person is crying, or there are kids screaming?
And there’s important policy work to do. How do good samaritan laws apply when an AI is giving the instructions? What regulatory frameworks do we need? Our colleague Mike Hogarth flagged this when we began our study: today, bystanders have strong legal protections when they perform CPR, but how those protections extend to AI-enabled CPR coaching is an open question that needs to be addressed.
MedicalResearch.com: Could a hospital-use model be developed?
Response: Absolutely. We focused on out-of-hospital cardiac arrest because that’s where the gap is most deadly — you’ve got untrained bystanders with no equipment. But the same approach could be adapted for in-hospital settings. Think about training medical students, nursing students, even experienced clinicians doing refresher training could use a system like this. It could also support code teams with scenario-specific guidance, especially in complex or unusual resuscitation situations. Pediatric codes, for example, have different protocols than adult codes, and even experienced providers can get tripped up on the specifics in a high-stress moment. The foundation we built is flexible enough to be adapted to those settings.
Citation:
Desai NMajhail NDredze M, et al. An Artificial Intelligence–Enabled Cardiopulmonary Resuscitation Instructor. JAMA Intern Med. Published online May 18, 2026. doi:10.1001/jamainternmed.2026.1552
Disclaimer: The information on MedicalResearch.com is provided for educational purposes only, and is in no way intended to diagnose, cure, or treat any medical or other condition. Some links are sponsored. Products, services and providers are not warranted or endorsed by MedicalResearch.com or Eminent Domains Inc. Always seek the advice of your physician or other qualified health and ask your doctor any questions you may have regarding a medical condition. In addition to all other limitations and disclaimers in this agreement, service provider and its third party providers disclaim any liability or loss in connection with the content provided on this website.
Last Updated on May 18, 2026 by Marie Benz MD FAAD