

07 Feb Geisinger Study: Methadone ‘take-homes’ during COVID-19 Resulted in Greater Methadone Overdoses
MedicalResearch.com Interview with:
Dr. Piper
Brian Piper, PhD MS
Assistant Professor of Neuroscience
Center for Pharmacy Innovation & Outcomes
Geisinger School of Graduate Education
MedicalResearch.com: What is the background for this study?
Response: Methadone is an evidence-based treatment of opioid use disorder (OUD) and pain. However, this Schedule II opioid can also cause respiratory depression, which can result in lethality. The need for supervised administration is a long-standing source of frustration in the U.S. for many opioid use disorder (OUD) methadone patients. However, there was an accommodation in early 2020 thanks to the COVID-19 pandemic. This involved extending the take-home supply to up to 28-days for stable patients and 14 days for less stable patients. Prior research found that the implementation of supervised administration in England greatly reduced methadone overdoses [1]. The primary objective of this study [2] from Geisinger Commonwealth School of Medicine was to determine if the relaxation of the take-home rules resulted in more methadone overdoses.
MedicalResearch.com: What are the main findings?
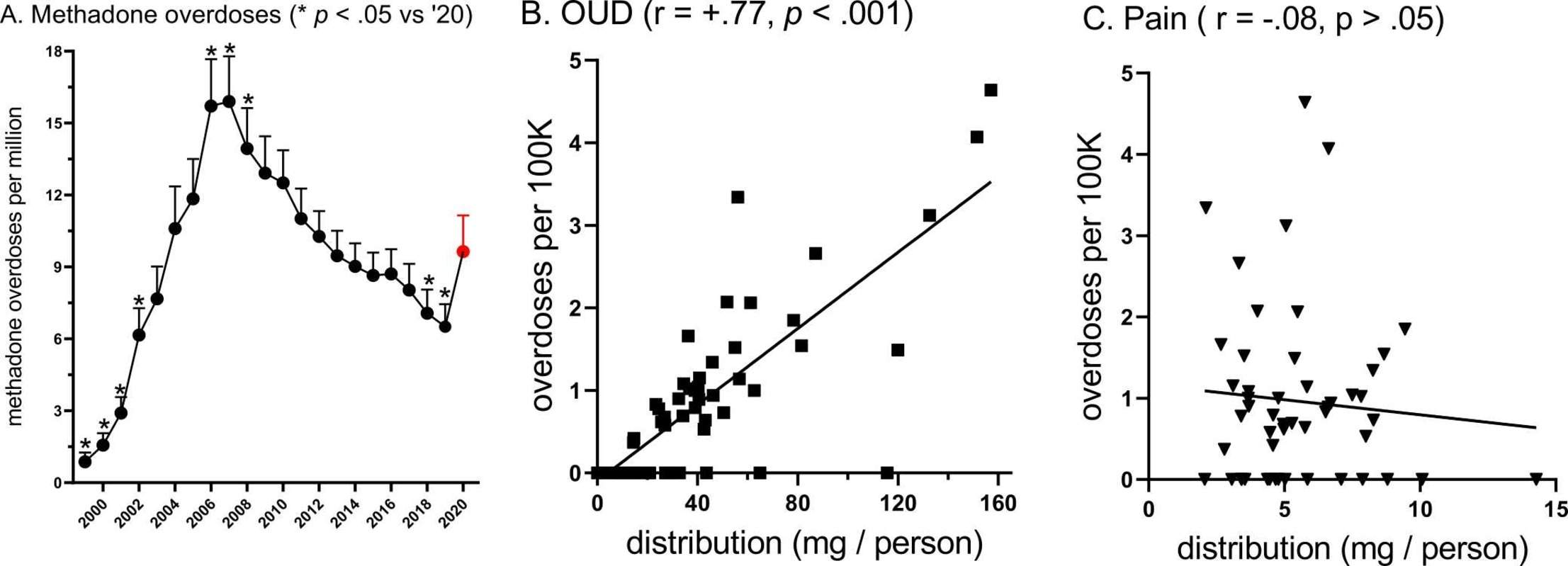
Response: Overdoses involving methadone from 1999 to 2020 were analyzed using data from the CDC’s WONDER database (Figure, left panel). There was a 48% increase from 2019 to 2020. Overdoses in 2020 were also significantly elevated relative to 2000–2003 and 2018 but significantly lower than 2006–2008. Among the top ten states for overdoses in 2020 (Rhode Island, Washington DC, Delaware, Connecticut, New Mexico, West Virginia, New York, Maine, Illinois, and Massachusetts), nine were located in the eastern US. New England states were also well represented.
The association between methadone overdoses and methadone distribution as reported by the Drug Enforcement Administration was also evaluated. The state level correlations between overall methadone use (r(49) = +0.75, p < .001), and opioid treatment program use (r(49) = +0.77, p < .001) with overdoses were positive, strong, and statistically significant (center panel). However, methadone use for pain treatment was not associated with methadone overdoses (r(49) = −0.08, right panel).
MedicalResearch.com: What should readers take away from your report?
Response: Accommodations for the COVID-19 pandemic were both well-intentioned and necessary. However, great caution should be made before making them permanent. There is value in supervised administration, particularly for OUD patients early in recovery, regular urine-analysis, and in-person counseling. We are concerned about turning our backs on past lessons in how to maximize the safety of methadone for OUD treatment [1]. These findings also contribute to a larger evidence base that methadone can be safely used for pain including cancer pain.
MedicalResearch.com: What recommendations do you have for future research as a results of this study?
Response: Death determination is made by both medical examiners and coroners and is not a simple process [3]. Further research on methadone involved overdoses should be completed by states with the resources to run the analytical chemistry including for other substances (e.g. xylazine) that may contribute to lethality. This study did not determine how many of the decedents were prescribed methadone versus how many purchased diverted methadone. As other reports indicate that there were 300K methadone patients and over 3,000 methadone overdoses in a single year (i.e. 1 overdose per 1,000 patients or 0.1% per year for a drug that many patients receive for multiple years), this topic should warrant further empirical attention.
MedicalResearch.com: Is there anything else you would like to add?
Response: Methadone, when combined with counseling, is an evidence-based treatment for opioid use disorder. Because methadone retains patients in treatment better than buprenorphine [4], it will continue to be an important component of biopsychosocial treatments for OUD.
Citations
- Strang J, et al. Impact of supervision of methadone consumption on deaths related to methadone overdose (1993-2008): Analyses using OD4 index in England and Scotland, BMJ 341 (2010) c4851.
- Kaufman et al. Examination of methadone involved overdoses during the COVID-19 pandemic. Forensic Science International 2023; 344:11579. https://authors.elsevier.com/a/1gXPQ1MCG0a4Rc
- Peppin et al. What your death certificate says about you may be wrong: A narrative review on CDC’s efforts to quantify prescription opioid overdose deaths. Cureus 2021; 13(9):e18012.
- Mattick et al. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2008; 2:CD002207,
Last Updated on February 7, 2023 by Marie Benz MD FAAD