[caption id="attachment_18793" align="alignleft" width="125"]

Dr. Franco[/caption]
MedicalResearch.com Interview with:
Dr. Pablo Moreno Franco MD
Assistant Professor of Medicine
MAYO Clinic
Medical Research: What is the background for this study? What are the main findings?
Dr. Pablo Franco: Early alerts and prompt management of patient with severe sepsis and septic shock (SS/S) starting in the emergency department (ED) have been shown to improve mortality and other pertinent outcomes. With this in mind, we formed a multidisciplinary sepsis and shock response team (SSRT) in September 2013. Automated electronic sniffer alerted ED providers for possible sepsis and when S/SS was identified, they were encouraged to activate SSRT.
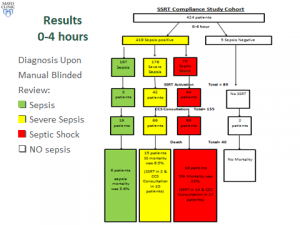
Two blinded reviewers retrospectively abstracted data on clinical trajectory and outcomes of all patients with sepsis and SS/S admitted at a single academic medical center between September 2013 and September 2014. Given importance of timely recognition and interventions in S/SS, we specifically focused on 2 periods: 0-4 hours and 4-12 hours after hospital admission. Additionally, we compared the compliance to “standard of care” between the SSRT pre-implementation period and the study period.
There were 167 patients admitted with
sepsis, among which there were 3 SSRT activations and sepsis mortality was 3.6%. There were 176 patients with SS, SSRT was called in 42 (23%) and SS mortality was 8.5%. CCS was involved in 66 patients and mortality was 6.9% if SSRT was activated, versus 21.6% if SSRT was not activated. There were 76 patients with septic shock, SSRT was called in 44 (57%) and septic shock mortality was 25%. Critical Care Service (CCS) was involved in 68 patients and mortality rates with and without SSRT were 30.9% and 15.4%, respectively. The all-or-none compliance with applicable goals of resuscitation improved from the baseline 0% to over 50% at the study period end. Overall observed/expected sepsis mortality index improved from 1.38 pre-SSRT to 0.68 post-SSRT implementation.

 Dr. Simone[/caption]
MedicalResearch.com Interview with:
Dr. Carmine Simone MD, FRCSC
Chief, Department of Surgery, Toronto East General Hospital
Co-Program Medical Director, Surgery HealthService, Toronto East General Hospital
Lecturer, University of Toronto, Division of Thoracic Surgery
Courtesy Staff, Sunnybrook Health Sciences Centre & Royal Victoria Hospital, Barrie
Medical Research: What is the background for this study? What are the main findings?
Dr. Simone: Patients preparing for surgery are often overwhelmed with information. Most of the time patients are given written instructions regarding preoperative preparation as well as written information at discharge. Our own institutional experience is that only 2/3 of patients read the information we provide and less than half of these patients can understand or retain the information they read.
We have found that providing patients SMS alerts or reminders leading up to their surgery increases the likelihood that they will follow instructions and keep their appointments. Furthermore having patients log their progress after discharged from hospital allows patients to track their progress and report complications earlier and avoid coming to the ER. Educational modules enable patients to better gauge their symptoms and make more informed decisions about calling the surgeon’s office or proceeding to the emergency department. We found a significant reduction in the number of ER visits and cancelled procedures after implementing the mobile device reminders and post-discharge daily log.
Dr. Simone[/caption]
MedicalResearch.com Interview with:
Dr. Carmine Simone MD, FRCSC
Chief, Department of Surgery, Toronto East General Hospital
Co-Program Medical Director, Surgery HealthService, Toronto East General Hospital
Lecturer, University of Toronto, Division of Thoracic Surgery
Courtesy Staff, Sunnybrook Health Sciences Centre & Royal Victoria Hospital, Barrie
Medical Research: What is the background for this study? What are the main findings?
Dr. Simone: Patients preparing for surgery are often overwhelmed with information. Most of the time patients are given written instructions regarding preoperative preparation as well as written information at discharge. Our own institutional experience is that only 2/3 of patients read the information we provide and less than half of these patients can understand or retain the information they read.
We have found that providing patients SMS alerts or reminders leading up to their surgery increases the likelihood that they will follow instructions and keep their appointments. Furthermore having patients log their progress after discharged from hospital allows patients to track their progress and report complications earlier and avoid coming to the ER. Educational modules enable patients to better gauge their symptoms and make more informed decisions about calling the surgeon’s office or proceeding to the emergency department. We found a significant reduction in the number of ER visits and cancelled procedures after implementing the mobile device reminders and post-discharge daily log.

