

25 May Thirty-fold state level prescribing disparities of naloxone to both Medicaid and Medicare patients
MedicalResearch.com Interview with:
Srivastava Kodavatiganti, MBS
Srivastava Kodavatiganti, MBS
Department of Medical Education
Geisinger Commonwealth School of Medicine
Scranton, PA
MedicalResearch.com: What is the background for this study?
Response: Prescription and illicit opioid misuse and overdoses have continued to escalate in the U.S. with annual overdoses exceeding 110,000[1]. There was a substantial rise from 2013 to 2022 in the number of opioid-related overdoses due to synthetic opioids [2]. Even nonfatal opioid-involved overdoses increased 4% quarterly between January 2018 and March 2022 as observed by encounters by emergency medical services [3]. Although the eastern U.S. has been particularly impacted by fatal overdoses, annual increases have increased as of last year in the western states including in Nevada (+27.9%), Washington (+36.9%), Oregon (+38.6%), and Alaska (+45.9%). In contrast, other states have seen more modest changes (New Mexico = +1.3%) including decreases (South Dakota = -2.4%, Nebraska = -19.5%) [1]. These findings underscore the importance for understanding patterns in usage of prevention and treatment strategies.
Naloxone is an opioid antagonist which can reverse the effects of an opioid overdose. This crucial lifesaving tool is administered as an injection or as a nasal spray. This study characterized the patterns of naloxone prescriptions in Medicaid patients from 2018 – 2021 and Medicare patients for 2019. State level differences were also quantified as the fold difference in prescribing between the highest and lowest states when correcting for the number of enrollees in each state.
MedicalResearch.com: What are the main findings?
Response: We saw that there was a difference between the number of prescriptions of brand name and generic naloxone. Brand name naloxone prescriptions increased by 245.1% while generic naloxone prescriptions decreased 5.3% from quarter 1 of 2018 to quarter 4 of 2021. The cost of prescriptions decreased modestly (-1.6%) for brand name naloxone and decreased by 14.6% for generic naloxone.
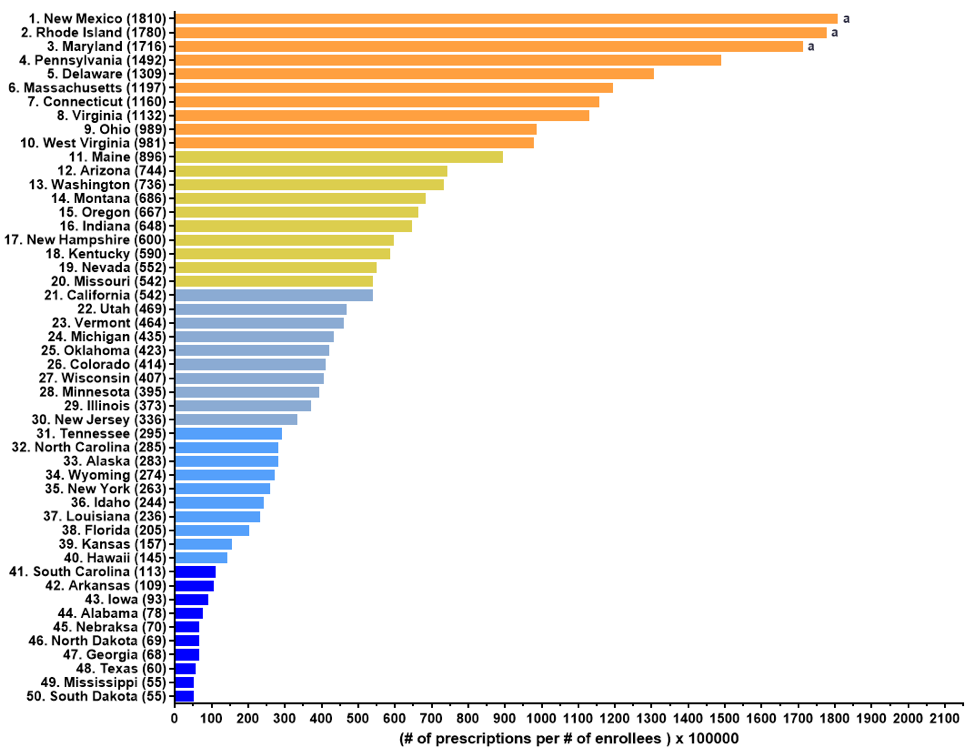
When evaluating state-by-state disparities, we found that the three highest prescribing states, New Mexico, Rhode Island, and Maryland, were outliers in quartile analysis for Medicaid claims in 2019. For 2019 Medicare claims, New Mexico, California, Tennessee, and Rhode Island were the highest prescribing states which were also found to be outliers. There was a moderate positive correlation (+0.47) with a double tail p value of 0.0006 in prescription rates between the Medicaid and Medicare programs.
A key finding of this novel study was that there was a 33.1-fold difference in Medicaid prescriptions between the highest (New Mexico = 1,809.5 prescriptions per one-hundred thousand enrollees) and lowest (South Dakota = 54.6) states in 2019. Similarly, Medicare saw a 30.4-fold difference in prescriptions between the highest (New Mexico=2,061.7) and lowest states (South Dakota = 67.8) [4].
Figure shows the pronounced state level differences in naloxone prescribing per one-hundred thousand Medicaid patients in 2019. States designated with an “a” were outliers in the quartile analysis that exceeded the upper limit of 1500 prescriptions per 100,000 enrollees
MedicalResearch.com: What should readers take away from your report?
Response: There was a substantial increase in overall naloxone prescriptions to Medicaid patients from 2018 to 2021. However, the increase in naloxone prescriptions was also accompanied by significant disparities between states. The large increase in Medicaid prescriptions could be attributable to insurance structure/policies and standing orders that benefit this population. When looking at the state-level disparities, stigma can play a role in determining access. Lastly, it is important for policymakers and pharmaceutical companies to consider financial barriers when determining the reimbursement rate and list price of this medication. Cost considerations including co-pays can restrict access. With the overall increase in claims, Medicaid coverage may be a strong determinant of accessibility to naloxone.
MedicalResearch.com: What recommendations do you have for future research as a result of this study?
Response: The thirty-fold disparities between states should be examined further to determine factors that drive these differences. In addition, it would bring further clarity on this topic to investigate the prescribers of naloxone in comparison to prescription rates, especially understanding if there was a difference between primary and specialty care, as well as any specific patient characteristics of interest. As both naloxone prescriptions [5] and drug overdoses [1] have been increasing nationally, it would be valuable to find what policy level factors, if any, are impactful at a state level in reducing non-fatal and fatal drug overdoses. Lastly, further studies can conclude if private versus public insurances also plays a factor in the temporal and state specific patterns.
Citations
[1] Centers for Disease Control and Prevention. Provisional drug overdose death counts. Accessed 4/20/2024 at: https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm
[2] Casillas SM, Pickens CM, Stokes EK, et al. Patient-level and county-level trends in nonfatal opioid-involved overdose emergency medical services encounters — 491 counties, United States, January 2018–March 2022. MMWR Morb Mortal Wkly Rep 2018;71:1073–80.
[3] Florence C, Luo F, Rice K. The economic burden of opioid use disorder and fatal opioid overdose in the United States, 2017. Drug & Alcohol Dependence 2021;218:108350.
[4] Manko CD, Ahmed MS, Harrison LR, et al. Retrospective study investigating naloxone
prescribing and cost in US Medicaid and Medicare patients. BMJ Open 2024;0:e078592. doi:10.1136/bmjopen-2023-078592
The information on MedicalResearch.com is provided for educational purposes only, and is in no way intended to diagnose, cure, or treat any medical or other condition. Always seek the advice of your physician or other qualified health and ask your doctor any questions you may have regarding a medical condition.
Some links may be sponsored.
In addition to all other limitations and disclaimers in this agreement, service provider and its third party providers disclaim any liability or loss in connection with the content provided on this website.
Last Updated on May 25, 2024 by Marie Benz MD FAAD