

02 Jul How Language Barriers Quietly Undermine Patient Safety
Posted at 09:58h
in Medical Translators
When a patient and clinician do not speak the same language, a routine visit can become unsafe. A symptom may be misunderstood. A medicine dose may be explained incorrectly. A patient may leave without knowing when to return, which warning signs require help, or how to follow the care plan.
These gaps are often hard to see. A nod can look like agreement even when the patient is confused, and a short answer may hide missing details. This is why qualified medical interpreters matter. They help patients and care teams exchange accurate information, ask questions, and confirm understanding before a decision is made.
Here, we look at how language barriers put patients at risk and why qualified medical interpreters matter.




 Maria Tan[/caption]
MedicalResearch.com:
Maria Y. Tian, MBS
Department of Medical Education
Geisinger College of Health Sciences
Scranton, Pennsylvania
MedicalResearch.com: What is the background for this study?
Response: Schizophrenia-spectrum disorders are severe, disabling conditions that are associated with substantial economic burden. Approximately one-third of patients have treatment-resistant schizophrenia, which clozapine is the only evidence-based therapy for. Clozapine also provides unique benefits, including reduced suicide risk, aggression, and all-cause mortality. Despite this, it has historically been underutilized due to concerns over adverse effects, required blood monitoring, patient adherence, and limited clinician training. Previous research in Medicaid populations had demonstrated marked state-level variation in use, but little was known about prescribing trends in the U.S. Medicare system, which covers nearly half of individuals with schizophrenia. This study analyzed Medicare Part D data from 2015–2020 to assess national and regional trends in clozapine prescribing and to identify states with significantly different prescribing patterns.
Maria Tan[/caption]
MedicalResearch.com:
Maria Y. Tian, MBS
Department of Medical Education
Geisinger College of Health Sciences
Scranton, Pennsylvania
MedicalResearch.com: What is the background for this study?
Response: Schizophrenia-spectrum disorders are severe, disabling conditions that are associated with substantial economic burden. Approximately one-third of patients have treatment-resistant schizophrenia, which clozapine is the only evidence-based therapy for. Clozapine also provides unique benefits, including reduced suicide risk, aggression, and all-cause mortality. Despite this, it has historically been underutilized due to concerns over adverse effects, required blood monitoring, patient adherence, and limited clinician training. Previous research in Medicaid populations had demonstrated marked state-level variation in use, but little was known about prescribing trends in the U.S. Medicare system, which covers nearly half of individuals with schizophrenia. This study analyzed Medicare Part D data from 2015–2020 to assess national and regional trends in clozapine prescribing and to identify states with significantly different prescribing patterns.





 Kalli Koukounas[/caption]
Kalli Koukounas, MPH
Kalli Koukounas[/caption]
Kalli Koukounas, MPH


 Kenya Colvin[/caption]
Kenya Colvin, MBS
Department of Medical Education
Scranton, PA
MedicalResearch.com: What is the background for this study?
Response: Vaccine hesitancy is a major driver of COVID-19 vaccination disparities between minority and non-Hispanic White communities. Our goal was to understand what factors influenced vaccine hesitancy among individuals in Eastern Pennsylvania to identify more effective ways to promote vaccine uptake within minority communities.
Kenya Colvin[/caption]
Kenya Colvin, MBS
Department of Medical Education
Scranton, PA
MedicalResearch.com: What is the background for this study?
Response: Vaccine hesitancy is a major driver of COVID-19 vaccination disparities between minority and non-Hispanic White communities. Our goal was to understand what factors influenced vaccine hesitancy among individuals in Eastern Pennsylvania to identify more effective ways to promote vaccine uptake within minority communities.






 Dr. Eberly[/caption]
Lauren A. Eberly, MD, MPH
Clinical Fellow, Cardiovascular Medicine
Perelman School of Medicine
Cardiovascular Division, Perelman School of Medicine
Center for Cardiovascular Outcomes, Quality, and Evaluative Research,
Cardiovascular Center for Health Equity and Social Justice,
Leonard Davis Institute of Health Economics
University of Pennsylvania, Philadelphia
MedicalResearch.com: What is the background for this study?
Response: Racial inequities are pervasive in our country, and cardiovascular therapeutics with proven benefit have been shown to be underutilized among Black and Latinx patients.
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs), a recommended treatment option for glycemic control in patients with diabetes, have recently emerged as a cardioprotective therapy as multiple large randomized clinical trials have shown they prevent cardiovascular events among patients with Type 2 Diabetes (T2D), particularly patients with established atherosclerotic cardiovascular disease (ASCVD). Given this, they are now recommended therapy for patients with diabetes and established or high risk of ASCVD.
Given the known inequitable utilization of other therapies, along with the known higher burden of diabetes and cardiovascular disease among Black patients, the aim of this study was to evaluate the uptake of GLP-1 RA as well as for inequities in utilization.
Dr. Eberly[/caption]
Lauren A. Eberly, MD, MPH
Clinical Fellow, Cardiovascular Medicine
Perelman School of Medicine
Cardiovascular Division, Perelman School of Medicine
Center for Cardiovascular Outcomes, Quality, and Evaluative Research,
Cardiovascular Center for Health Equity and Social Justice,
Leonard Davis Institute of Health Economics
University of Pennsylvania, Philadelphia
MedicalResearch.com: What is the background for this study?
Response: Racial inequities are pervasive in our country, and cardiovascular therapeutics with proven benefit have been shown to be underutilized among Black and Latinx patients.
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs), a recommended treatment option for glycemic control in patients with diabetes, have recently emerged as a cardioprotective therapy as multiple large randomized clinical trials have shown they prevent cardiovascular events among patients with Type 2 Diabetes (T2D), particularly patients with established atherosclerotic cardiovascular disease (ASCVD). Given this, they are now recommended therapy for patients with diabetes and established or high risk of ASCVD.
Given the known inequitable utilization of other therapies, along with the known higher burden of diabetes and cardiovascular disease among Black patients, the aim of this study was to evaluate the uptake of GLP-1 RA as well as for inequities in utilization. 
 Dr. Ashwin Nathan[/caption]
Ashwin Nathan, MD, MSHP
Assistant Professor, Medicine, Perelman School of Medicine
Interventional Cardiologist
Hospital of the University of Pennsylvania and at the
Corporal Michael C. Crescenz VA Medical Center in Philadelphia
Penn Cardiovascular Outcomes, Quality & Evaluative Research Center
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: We found that the rates of TAVR were lower in areas with higher proportions of Black, Hispanic and socioeconomically disadvantaged patients. Inequities in access in areas with higher proportions of Black and Hispanic patients existed despite adjusting for socioeconomic status.
Dr. Ashwin Nathan[/caption]
Ashwin Nathan, MD, MSHP
Assistant Professor, Medicine, Perelman School of Medicine
Interventional Cardiologist
Hospital of the University of Pennsylvania and at the
Corporal Michael C. Crescenz VA Medical Center in Philadelphia
Penn Cardiovascular Outcomes, Quality & Evaluative Research Center
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: We found that the rates of TAVR were lower in areas with higher proportions of Black, Hispanic and socioeconomically disadvantaged patients. Inequities in access in areas with higher proportions of Black and Hispanic patients existed despite adjusting for socioeconomic status.



 Dr. Cole[/caption]
Megan B. Cole, PhD, MPH
Assistant Professor | Dept. of Health Law, Policy, & Management
Co-Director | BU Medicaid Policy Lab
Boston University School of Public Health
Boston, MA 02118
MedicalResearch.com: What is the background for this study?
Response: Under the Affordable Care Act, states were given the option to expand Medicaid eligibility to nonelderly adults with incomes up to 138% of the federal poverty level, where in January 2014, 25 states plus Washington, DC expanded eligibility, with 13 additional states expanding thereafter. State Medicaid expansion decisions were particularly consequential for federally qualified health centers (FQHCs), which serve nearly 30 million low-income, disproportionately uninsured patients across the US.
We know from earlier work that in the shorter-term, Medicaid expansion was associated with improvements in quality of care process measures and FQHC service capacity. However, we conducted the first known nationally representative study to examine how Medicaid expansion impacted key chronic disease outcome measures at FQHCs over the longer-term by looking at changes five years after implementation, including changes by race/ethnicity.
Dr. Cole[/caption]
Megan B. Cole, PhD, MPH
Assistant Professor | Dept. of Health Law, Policy, & Management
Co-Director | BU Medicaid Policy Lab
Boston University School of Public Health
Boston, MA 02118
MedicalResearch.com: What is the background for this study?
Response: Under the Affordable Care Act, states were given the option to expand Medicaid eligibility to nonelderly adults with incomes up to 138% of the federal poverty level, where in January 2014, 25 states plus Washington, DC expanded eligibility, with 13 additional states expanding thereafter. State Medicaid expansion decisions were particularly consequential for federally qualified health centers (FQHCs), which serve nearly 30 million low-income, disproportionately uninsured patients across the US.
We know from earlier work that in the shorter-term, Medicaid expansion was associated with improvements in quality of care process measures and FQHC service capacity. However, we conducted the first known nationally representative study to examine how Medicaid expansion impacted key chronic disease outcome measures at FQHCs over the longer-term by looking at changes five years after implementation, including changes by race/ethnicity.



 Dr. Correa[/caption]
Andres F. Correa, MD
Assistant Professor
Department of Surgical Oncology, and
[caption id="attachment_57815" align="alignleft" width="150"]
Dr. Correa[/caption]
Andres F. Correa, MD
Assistant Professor
Department of Surgical Oncology, and
[caption id="attachment_57815" align="alignleft" width="150"] Dr. Bernstein[/caption]
Adrien Bernstein, MD
Second Year Urologic Oncology Fellow
Fox Chase Cancer Center
MedicalResearch.com: What is the background for this study?
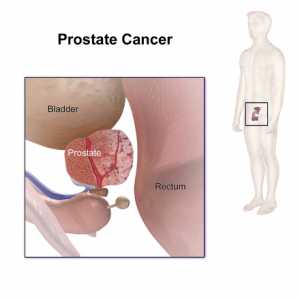
Response: Unfortunately, it has been well-established that historically Black Americans experience increased cancer specific mortality compared to white patients. In prostate cancer specifically studies have shown that when access to care is equitable this gap resolves. This suggests that biological factors are not driving these differences but rather the result of the complex interplay of social determinants and systemic inequities in our healthcare system.
Early in the pandemic, multiple studies demonstrated that minority communities disproportionately shouldered poor COVID-19 outcomes. On March 13th 2020, the American College of Surgeons recommended against elective procedures; however, the definition of an elective oncologic case was left to the discretion of the provider. As prostate cancer treatment can be safely deferred up to a year follow diagnosis, management of prostate cancer during the initial lockdown period of the COVID-19 Pandemic provided a useful analysis of the differential restrictions placed on non-emergent health care during the Pandemic.
Dr. Bernstein[/caption]
Adrien Bernstein, MD
Second Year Urologic Oncology Fellow
Fox Chase Cancer Center
MedicalResearch.com: What is the background for this study?
Response: Unfortunately, it has been well-established that historically Black Americans experience increased cancer specific mortality compared to white patients. In prostate cancer specifically studies have shown that when access to care is equitable this gap resolves. This suggests that biological factors are not driving these differences but rather the result of the complex interplay of social determinants and systemic inequities in our healthcare system.
Early in the pandemic, multiple studies demonstrated that minority communities disproportionately shouldered poor COVID-19 outcomes. On March 13th 2020, the American College of Surgeons recommended against elective procedures; however, the definition of an elective oncologic case was left to the discretion of the provider. As prostate cancer treatment can be safely deferred up to a year follow diagnosis, management of prostate cancer during the initial lockdown period of the COVID-19 Pandemic provided a useful analysis of the differential restrictions placed on non-emergent health care during the Pandemic. 


