For many years now, professional nursing has held a unique place in the American health care system. Nurses make up one of the largest health care professions in the U.S. with more than 3.1 million nurses working in diverse fields and settings.
Although most nurses work in health care settings like hospitals, a nurse’s expertise expands well beyond the hospital walls. Working on their own and alongside other healthcare professionals, nurses promote the health of families, individuals, and communities.
Nurses have always played an important role in healthcare settings. However, their role has changed a lot over the years. In the past, nurses had extraordinarily little formal medical training. In fact, nurses learned the medical skills they needed from their mothers or other women in the nursing profession.
Today, the nursing profession has changed for the better. Not only are there extensive training programs available for nurses, but this role now comes with a level of prestige that was not there before. And this is not the only thing that has altered. Technology has also played a huge role in changing this profession for the better. Keep reading below to find out about the history of nursing and how technology has changed the role of nursing. For those seeking additional assistance or support in navigating the complexities of nursing education or academic tasks, exploring resources from reputable
nursing paper writing services can offer valuable expertise and assistance in achieving success in the field.
How Nursing Has Changed Over Time
Time has done a lot for many career paths. However, the nursing profession has seen more changes than most. Here are some of the ways the nursing profession has changed over time:
Training – in the past, nurses were not required to have any formal education. However, nowadays nurses are no longer able to care for patients without passing the correct certification first.
Setting – many years ago, nurses would take care of people in their homes or on the battlefield. Although some nurses still care for patients in their homes, nowadays, most nurses work in a hospital setting.
Responsibilities – nursing responsibilities have come a long way from the early days when they used to look a lot like a household chore list. The change in responsibilities for nurses stems from several changes in the profession, including the changing views of women, more comprehensive training, and the growing demand for medical professionals.
Culture – in the 20
th century, nursing culture was known as being mainly made up of females who had a small amount of medical knowledge. While nursing culture has not changed completely, it has changed a lot over the years. In fact, research suggests that more men than ever are choosing to train in this profession.
Patient care – patient care is more important than ever before. The advancements in technology have created an environment that makes patient care more helpful and efficient for patients. These advancements have altered almost every industry in the U.S. and the medical field is no different.






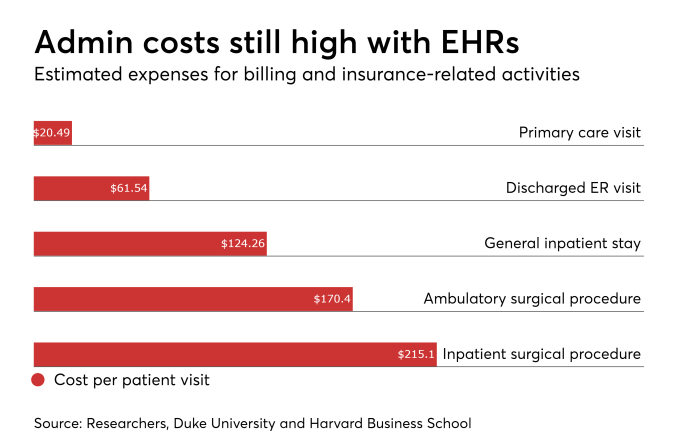
 The healthcare system generates an extraordinary volume of structured data. The United States alone produces approximately 1.2 billion clinical care documents annually. Managing that volume has become one of the most significant operational challenges in modern medicine, consuming physician time at a rate that directly affects patient care quality.
AI and automation are increasingly positioned as the most scalable solution. The question is no longer whether technology will reshape clinical documentation workflows, but how rapidly health systems can implement it responsibly.
The healthcare system generates an extraordinary volume of structured data. The United States alone produces approximately 1.2 billion clinical care documents annually. Managing that volume has become one of the most significant operational challenges in modern medicine, consuming physician time at a rate that directly affects patient care quality.
AI and automation are increasingly positioned as the most scalable solution. The question is no longer whether technology will reshape clinical documentation workflows, but how rapidly health systems can implement it responsibly.