
 Dr. Garcia-De-Albeniz[/caption]
Xabier Garcia-De-Albeniz MD PhD
Research Associate
Department of Epidemiology
Harvard T.H. Chan School of Public Health
Mongan Institute for Health Policy
Massachusetts General Hospital
MedicalResearch.com: What is the background for this study?
Response: The goal of breast cancer screening is to reduce deaths from breast cancer by finding breast cancer at early, more treatable stages. The main way to screen for breast cancer is periodic mammography, which is an x-ray of the breast that can show tumors before they are large enough to feel. High-quality studies called clinical trials have shown that screening women in their 50s and 60s decreases breast cancer deaths. However, the point at which women can safely stop screening because it no longer decreases breast cancer deaths has not been studied. More than half of women in the United States continue screening mammography after age 75 years.
Dr. Garcia-De-Albeniz[/caption]
Xabier Garcia-De-Albeniz MD PhD
Research Associate
Department of Epidemiology
Harvard T.H. Chan School of Public Health
Mongan Institute for Health Policy
Massachusetts General Hospital
MedicalResearch.com: What is the background for this study?
Response: The goal of breast cancer screening is to reduce deaths from breast cancer by finding breast cancer at early, more treatable stages. The main way to screen for breast cancer is periodic mammography, which is an x-ray of the breast that can show tumors before they are large enough to feel. High-quality studies called clinical trials have shown that screening women in their 50s and 60s decreases breast cancer deaths. However, the point at which women can safely stop screening because it no longer decreases breast cancer deaths has not been studied. More than half of women in the United States continue screening mammography after age 75 years.
 Dr. Kressin[/caption]
Nancy R. Kressin, PhD
VA Medical Center, Jamaica Plain Campus
Boston, MA
MedicalResearch.com: What is the background for this study?
Response: State-level legislation requires informing women about breast density (BD) with mammogram results, to increase awareness of BD’s tendency to mask cancers on mammography, its association with increased breast cancer risk, and to encourage women to discuss personal risk and supplemental screening with physicians.
The Food and Drug Administration is currently developing dense breast notification (DBN) language for use nationwide; information about effects of state DBNs could be informative for FDA’s language.
Dr. Kressin[/caption]
Nancy R. Kressin, PhD
VA Medical Center, Jamaica Plain Campus
Boston, MA
MedicalResearch.com: What is the background for this study?
Response: State-level legislation requires informing women about breast density (BD) with mammogram results, to increase awareness of BD’s tendency to mask cancers on mammography, its association with increased breast cancer risk, and to encourage women to discuss personal risk and supplemental screening with physicians.
The Food and Drug Administration is currently developing dense breast notification (DBN) language for use nationwide; information about effects of state DBNs could be informative for FDA’s language.
 Dr. Moorman[/caption]
Sarah Moorman, MD
Department of Radiology
Michigan Medicine
MedicalResearch.com: What is the background for this study?
Response: Professional societies and government agencies have variable recommendations regarding how often women should get a screening mammogram. Breast cancer screening may be recommended annually or biennially. These differing recommendations lead to confusion for both referring physicians and patients.
The goal of our study was to better understand differences between annual and biennial screening. We reviewed clinical outcomes of women undergoing annual or biennial mammographic screening to determine if there is an advantage to annual screening.
Dr. Moorman[/caption]
Sarah Moorman, MD
Department of Radiology
Michigan Medicine
MedicalResearch.com: What is the background for this study?
Response: Professional societies and government agencies have variable recommendations regarding how often women should get a screening mammogram. Breast cancer screening may be recommended annually or biennially. These differing recommendations lead to confusion for both referring physicians and patients.
The goal of our study was to better understand differences between annual and biennial screening. We reviewed clinical outcomes of women undergoing annual or biennial mammographic screening to determine if there is an advantage to annual screening.
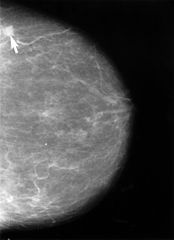
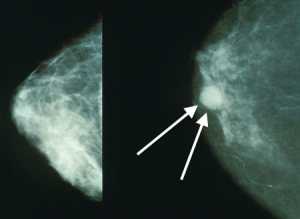 Mammograms showing a normal breast (left) and a breast with cancer (right, white arrows). Wikipedia Image[/caption]
Dr. Elham Kharazmi, MD, PhD
Co-Leader, Risk Adapted Prevention (RAD) Group
Division of Preventive Oncology
National Center for Tumor Diseases (NCT)
German Cancer Research Center (DKFZ)
Germany
MedicalResearch.com: What is the background for this study?
Response: Breast cancer is the most common cancer in women worldwide and the second leading cause of cancer death in American women, exceeded only by lung cancer. Available evidence suggests that implementation of a screening program can decrease breast cancer mortality.
Reductions in breast cancer mortality in Europe over the past two decades have been associated at least in part with the implementation of screening programs. Screening enables the detection of tumors at an early stage, when more treatment options are feasible and most effective. However, screening is associated with substantial risks, such as over-diagnosis, false-positive results, and physical and psychological harms, particularly when large numbers of women with low risk are frequently screened.
Mammograms showing a normal breast (left) and a breast with cancer (right, white arrows). Wikipedia Image[/caption]
Dr. Elham Kharazmi, MD, PhD
Co-Leader, Risk Adapted Prevention (RAD) Group
Division of Preventive Oncology
National Center for Tumor Diseases (NCT)
German Cancer Research Center (DKFZ)
Germany
MedicalResearch.com: What is the background for this study?
Response: Breast cancer is the most common cancer in women worldwide and the second leading cause of cancer death in American women, exceeded only by lung cancer. Available evidence suggests that implementation of a screening program can decrease breast cancer mortality.
Reductions in breast cancer mortality in Europe over the past two decades have been associated at least in part with the implementation of screening programs. Screening enables the detection of tumors at an early stage, when more treatment options are feasible and most effective. However, screening is associated with substantial risks, such as over-diagnosis, false-positive results, and physical and psychological harms, particularly when large numbers of women with low risk are frequently screened.
 Philippe Henrot, MD
Radiology Department
Institut de Cancerologie de Lorraine
Vandoeuvre-les-Nancy
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: The initial observation was that daily practice of mammography shows a substantial proportion of women that report a negative experience after having a mammogram. Compression of the breast before delivering X-rays is mandatory to achieve the best image quality and to detect small cancers. Unfortunately, compression is uncomfortable, even sometimes painful.
We took into consideration a study of PJ Kornguth et al. published in 1993 reporting the self-compression technique. In this study one breast was compressed by the radiographer and the other with self-compression. The author reported a high level of patient satisfaction, and a lower discomfort, without compromising image quality. We performed a multicenter prospective randomized trial to demonstrate the feasibility of the self-compression technique in condition similar to routine screening or follow-up, compared with standard compression. The primary outcome was to demonstrate that self-compression did not lead to compress the breast less than standard compression, and that was done. The secondary outcomes were to evaluate pain, compression force and image quality.
The results indicated that compression force was higher when the women controlled themselves the compression of their breast, and the pain measured on a visual analogue scale was lower. Moreover, image quality was not compromised compared with standard compression.
Philippe Henrot, MD
Radiology Department
Institut de Cancerologie de Lorraine
Vandoeuvre-les-Nancy
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: The initial observation was that daily practice of mammography shows a substantial proportion of women that report a negative experience after having a mammogram. Compression of the breast before delivering X-rays is mandatory to achieve the best image quality and to detect small cancers. Unfortunately, compression is uncomfortable, even sometimes painful.
We took into consideration a study of PJ Kornguth et al. published in 1993 reporting the self-compression technique. In this study one breast was compressed by the radiographer and the other with self-compression. The author reported a high level of patient satisfaction, and a lower discomfort, without compromising image quality. We performed a multicenter prospective randomized trial to demonstrate the feasibility of the self-compression technique in condition similar to routine screening or follow-up, compared with standard compression. The primary outcome was to demonstrate that self-compression did not lead to compress the breast less than standard compression, and that was done. The secondary outcomes were to evaluate pain, compression force and image quality.
The results indicated that compression force was higher when the women controlled themselves the compression of their breast, and the pain measured on a visual analogue scale was lower. Moreover, image quality was not compromised compared with standard compression.

 Dr. Newman[/caption]
Lisa A Newman, MD
Director of the Breast Oncology Program for the multi-hospital
Henry Ford Health System
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: In 2009 the United States Preventive Services Task Force published a guideline recommending that American women at average risk for breast cancer defer undergoing screening mammography until they reach the age of 50 years. Prior to this publication, women were widely-encouraged to initiate annual mammography at age 40 years. Women that have a history of breast cancer are automatically considered to be at increased risk for developing a new breast cancer, and so routine screening mammography guidelines do not apply to them. These women require annual mammography regardless of age, unless they have undergone a bilateral mastectomy.
We utilized data from Michigan Blue Cross/Blue Shield to evaluate patterns of mammography utilization among women age 40-49 years, comparing rates before versus after 2009, when the USPSTF guideline was published. We analyzed women that had a prior history of breast cancer separately from those that had no history of breast cancer, and we excluded women that underwent bilateral mastectomy.
Disturbingly, we found that mammography utilization rates declined among women with a history of breast cancer as well as among those with no history of breast cancer in the post-2009 timeline.
This suggested to us that changes in screening recommendations may have had the unintended consequence of generating confusion and misunderstandings regarding the value of mammography among women that undeniably benefit from this imaging, such as those with a history of breast cancer.
Dr. Newman[/caption]
Lisa A Newman, MD
Director of the Breast Oncology Program for the multi-hospital
Henry Ford Health System
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: In 2009 the United States Preventive Services Task Force published a guideline recommending that American women at average risk for breast cancer defer undergoing screening mammography until they reach the age of 50 years. Prior to this publication, women were widely-encouraged to initiate annual mammography at age 40 years. Women that have a history of breast cancer are automatically considered to be at increased risk for developing a new breast cancer, and so routine screening mammography guidelines do not apply to them. These women require annual mammography regardless of age, unless they have undergone a bilateral mastectomy.
We utilized data from Michigan Blue Cross/Blue Shield to evaluate patterns of mammography utilization among women age 40-49 years, comparing rates before versus after 2009, when the USPSTF guideline was published. We analyzed women that had a prior history of breast cancer separately from those that had no history of breast cancer, and we excluded women that underwent bilateral mastectomy.
Disturbingly, we found that mammography utilization rates declined among women with a history of breast cancer as well as among those with no history of breast cancer in the post-2009 timeline.
This suggested to us that changes in screening recommendations may have had the unintended consequence of generating confusion and misunderstandings regarding the value of mammography among women that undeniably benefit from this imaging, such as those with a history of breast cancer.

 Dr. Horný[/caption]
Michal Horný PhD
Assistant Professor
Emory University School of Medicine, Department of Radiology and Imaging Sciences
Emory University Rollins School of Public Health
Department of Health Policy and Management
Atlanta, GA 30322
MedicalResearch.com: What is the background for this study?
Response: Increased breast tissue density is a common finding at screening mammography. Approximately 30-50% of women have so-called “dense breasts” but many of them are not aware of it. The problem is that the increased tissue density can potentially mask early cancers. In other words, if there is cancer hiding in dense breast tissue, it could be difficult to spot it.
To improve the awareness of breast tissue density, a patient group called Are You Dense Advocacy, Inc., started lobbying state and federal policymakers to pass laws mandating health care providers to notify women about their breast density assessments. As a result, 31 states have already enacted some form of legislation regarding dense breast tissue.
Dr. Horný[/caption]
Michal Horný PhD
Assistant Professor
Emory University School of Medicine, Department of Radiology and Imaging Sciences
Emory University Rollins School of Public Health
Department of Health Policy and Management
Atlanta, GA 30322
MedicalResearch.com: What is the background for this study?
Response: Increased breast tissue density is a common finding at screening mammography. Approximately 30-50% of women have so-called “dense breasts” but many of them are not aware of it. The problem is that the increased tissue density can potentially mask early cancers. In other words, if there is cancer hiding in dense breast tissue, it could be difficult to spot it.
To improve the awareness of breast tissue density, a patient group called Are You Dense Advocacy, Inc., started lobbying state and federal policymakers to pass laws mandating health care providers to notify women about their breast density assessments. As a result, 31 states have already enacted some form of legislation regarding dense breast tissue.

MedicalResearch.com Interview with:
[caption id="attachment_42920" align="alignleft" width="150"] Dr. Pashayan[/caption]
Dr Nora Pashayan PhD
Clinical Reader in Applied Health Research
University College London
Dept of Applied Health Research
London
MedicalResearch.com: What is the background for this study?
Response: Not all women have the same risk of developing breast cancer and not all women have the same potential to benefit from screening.
If the screening programme takes into account the individual variation in risk, then evidence from different studies indicate that this could improve the efficiency of the screening programme. However, questions remain on what is the best risk-stratified screening strategy, does risk-stratified screening add value for money, and what are benefit and harm trade-offs.
 Prof. Duffy[/caption]
Prof. Duffy[/caption]
Stephen W. Duffy Professor of Cancer Screening Wolfson Institute of Preventive Medicine, Barts and The London School of Medicine and Dentistry Queen Mary University of London
MedicalResearch.com: What is the background for this study? What are the main findings? Response: The phenomenon of length bias, whereby screening has more chance of detecting slow growing tumours, has been known about for some years. This has led some colleagues to speculate that breast cancer screening only benefits those with slow-growing, less aggressive cancers, and does not reduce deaths from more aggressive, rapidly progressing cancers. In this study, we addressed this question directly using data from a randomised trial of mammographic screening. We calculated the reduction in mortality from grade 1 (less aggressive), grade 2 (intermediate) and grade 3 (most aggressive) cancers, as a result of screening. We found that the greatest reduction in breast cancer mortality was from the aggressive, fast-growing grade 3 cancers, contrary to what had been suspected. Dr. Bahl[/caption]
Manisha Bahl, MD, MPH
Director, Breast Imaging Fellowship Program,
Massachusetts General Hospital
Assistant Professor of Radiology,
Harvard Medical School
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Image-guided biopsies that we perform based on suspicious findings on mammography can yield one of three pathology results: cancer, high-risk, or benign. Most high-risk breast lesions are noncancerous, but surgical excision is typically recommended because some high-risk lesions can be upgraded to cancer at surgery. Currently, there are no imaging or other features that reliably allow us to distinguish between high-risk lesions that warrant surgery from those that can be safely followed, which has led to unnecessary surgery of high-risk lesions that are not associated with cancer.
We decided to apply machine learning algorithms to help us with this challenging clinical scenario: to distinguish between high-risk lesions that warrant surgery from those that can be safely followed. Machine learning allows us to incorporate the full spectrum of diverse and complex data that we have available, such as patient risk factors and imaging features, in order to predict which high-risk lesions are likely to be upgraded to cancer and, ultimately, to help our patients make more informed decisions about surgery versus surveillance.
We developed the machine learning model with almost 700 high-risk lesions, then tested it with more than 300 high-risk lesions. Instead of surgical excision of all high-risk lesions, if those categorized with the model to be at low risk for upgrade were surveilled and the remainder were excised, then 97.4% malignancies would have been diagnosed at surgery, and 30.6% of surgeries of benign lesions could have been avoided.
Mammogram showing small lesion
Dr. Bahl[/caption]
Manisha Bahl, MD, MPH
Director, Breast Imaging Fellowship Program,
Massachusetts General Hospital
Assistant Professor of Radiology,
Harvard Medical School
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Image-guided biopsies that we perform based on suspicious findings on mammography can yield one of three pathology results: cancer, high-risk, or benign. Most high-risk breast lesions are noncancerous, but surgical excision is typically recommended because some high-risk lesions can be upgraded to cancer at surgery. Currently, there are no imaging or other features that reliably allow us to distinguish between high-risk lesions that warrant surgery from those that can be safely followed, which has led to unnecessary surgery of high-risk lesions that are not associated with cancer.
We decided to apply machine learning algorithms to help us with this challenging clinical scenario: to distinguish between high-risk lesions that warrant surgery from those that can be safely followed. Machine learning allows us to incorporate the full spectrum of diverse and complex data that we have available, such as patient risk factors and imaging features, in order to predict which high-risk lesions are likely to be upgraded to cancer and, ultimately, to help our patients make more informed decisions about surgery versus surveillance.
We developed the machine learning model with almost 700 high-risk lesions, then tested it with more than 300 high-risk lesions. Instead of surgical excision of all high-risk lesions, if those categorized with the model to be at low risk for upgrade were surveilled and the remainder were excised, then 97.4% malignancies would have been diagnosed at surgery, and 30.6% of surgeries of benign lesions could have been avoided.
Mammogram showing small lesion Dr. Karla Evans[/caption]
Karla K. Evans, Ph.D.
Lecturer, Department of Psychology
The University of York
Heslington, York UK
MedicalResearch.com: What is the background for this study?
Response: This research started after initially talking to radiologists and pathologists about how they search a radiograph or micrograph for abnormalities. They talked about being able to tell at the first glance if the image had something bad about it. Jokingly, they talked about “having the force” to see the bad. We wanted to know whether this hunch after the brief initial viewing was real and to systematically test it. We collected radiographic and micrographic images, half of them that had signs of cancer in them and half of them that didn't, and we briefly presented them (250 millisecond to 2000 milliseconds) to radiologists or pathologistsrespectively. They simply had to report whether they would recall the patient or not and try localize on the outline the location of the abnormality. We first reported these finding in the following paper.
Evans et al. (2013) The Gist of the Abnormal: Above chance medical decision making in the blink of an eye. Psychonomic Bulletin & Review (DOI) 10.3758/s13423-013-0459-3
In addition to finding that radiologists and pathologists can indeed detect subtle cancers in a quarter of a second we also found that they did not know where it was in the image leading us to conclude that the signal that they were picking up must be a global signal (i.e. the global image statistic or the texture of the breast as a whole) rather than the result of a local saliency. This led me to start further exploring this signal in order to characterize it when I moved to University or York, UK to establish my own lab.
Dr. Karla Evans[/caption]
Karla K. Evans, Ph.D.
Lecturer, Department of Psychology
The University of York
Heslington, York UK
MedicalResearch.com: What is the background for this study?
Response: This research started after initially talking to radiologists and pathologists about how they search a radiograph or micrograph for abnormalities. They talked about being able to tell at the first glance if the image had something bad about it. Jokingly, they talked about “having the force” to see the bad. We wanted to know whether this hunch after the brief initial viewing was real and to systematically test it. We collected radiographic and micrographic images, half of them that had signs of cancer in them and half of them that didn't, and we briefly presented them (250 millisecond to 2000 milliseconds) to radiologists or pathologistsrespectively. They simply had to report whether they would recall the patient or not and try localize on the outline the location of the abnormality. We first reported these finding in the following paper.
Evans et al. (2013) The Gist of the Abnormal: Above chance medical decision making in the blink of an eye. Psychonomic Bulletin & Review (DOI) 10.3758/s13423-013-0459-3
In addition to finding that radiologists and pathologists can indeed detect subtle cancers in a quarter of a second we also found that they did not know where it was in the image leading us to conclude that the signal that they were picking up must be a global signal (i.e. the global image statistic or the texture of the breast as a whole) rather than the result of a local saliency. This led me to start further exploring this signal in order to characterize it when I moved to University or York, UK to establish my own lab.
 Brian L. Sprague, PhD
Assistant Professor
Department of Surgery
Assistant Professor
Department of Biochemistry
University of Vermont
MedicalResearch.com: What is the background for this study?
Response: Having dense breasts makes mammography more difficult to interpret and is also an independent risk factor for developing breast cancer. About half of all U.S. states require that information on the density of a woman's breasts be made available to her after a mammogram, and in some states the report must also inform such women that there are additional tests, such as breast magnetic resonance imaging (MRI), that may detect breast cancer in women who have dense breasts and normal mammograms.
Such laws are controversial because of the large number of women affected (around 40% of women aged 40-74) and due to a lack of consensus in the medical community regarding the benefits and harms of supplemental screening strategies. An additional concern is the subjective nature of breast density assessment, which is based on the Breast Imaging Reporting and Data System (BI-RADS) that provides four possible categories for breast density.
Brian L. Sprague, PhD
Assistant Professor
Department of Surgery
Assistant Professor
Department of Biochemistry
University of Vermont
MedicalResearch.com: What is the background for this study?
Response: Having dense breasts makes mammography more difficult to interpret and is also an independent risk factor for developing breast cancer. About half of all U.S. states require that information on the density of a woman's breasts be made available to her after a mammogram, and in some states the report must also inform such women that there are additional tests, such as breast magnetic resonance imaging (MRI), that may detect breast cancer in women who have dense breasts and normal mammograms.
Such laws are controversial because of the large number of women affected (around 40% of women aged 40-74) and due to a lack of consensus in the medical community regarding the benefits and harms of supplemental screening strategies. An additional concern is the subjective nature of breast density assessment, which is based on the Breast Imaging Reporting and Data System (BI-RADS) that provides four possible categories for breast density.
 Dr. Rachel Brem[/caption]
Rachel Brem, MD
Professor of Radiology and
Director of Breast Imaging and Intervention
George Washington University School of Medicine.
MedicalResearch.com Editor’s note: Many states now have laws regarding patient notification of breast density after mammography screening.
Dr. Brem discusses the background and implications of the new mandatory notification laws.
MedicalResearch.com: What is meant by 'breast density?’ Is breast density a risk factor for breast cancer? Is breast cancer more difficult to detect in dense breasts?
Dr. Brem: Breast density is a measure used to describe the proportion of fat versus breast tissue, which includes fibrous and glandular tissue. Dense breasts contain more fibrous and glandular tissue and less fatty tissue. This is important because on a mammogram dense breast tissue is white and breast cancer is white. The lack of contrast can make detecting cancer more difficult.
You can only tell if your breasts are dense from the mammogram. You can’t feel dense breast tissue or see it.
An estimated 40 percent of women have dense breast tissue that may mask the presence of cancerous tissue in standard mammography. Dense breast tissue decreases with age, but remains important throughout life. Over 75 percent of women in their 40s have dense breast tissue but over a third of women in their 70s have dense breast tissue.
As breast density increases, mammography sensitivity decreases. This is significant, but we must consider the increased risk of breast cancer in women with dense breast tissue. Women with dense breast tissue have up to a four-fold increased risk of developing breast cancer. So, breast density is essentially the “perfect storm” where the ability to detect cancer decreases while the risk for breast cancer increases. Therefore, optimal approaches to individualized breast cancer screening are needed.
Dr. Rachel Brem[/caption]
Rachel Brem, MD
Professor of Radiology and
Director of Breast Imaging and Intervention
George Washington University School of Medicine.
MedicalResearch.com Editor’s note: Many states now have laws regarding patient notification of breast density after mammography screening.
Dr. Brem discusses the background and implications of the new mandatory notification laws.
MedicalResearch.com: What is meant by 'breast density?’ Is breast density a risk factor for breast cancer? Is breast cancer more difficult to detect in dense breasts?
Dr. Brem: Breast density is a measure used to describe the proportion of fat versus breast tissue, which includes fibrous and glandular tissue. Dense breasts contain more fibrous and glandular tissue and less fatty tissue. This is important because on a mammogram dense breast tissue is white and breast cancer is white. The lack of contrast can make detecting cancer more difficult.
You can only tell if your breasts are dense from the mammogram. You can’t feel dense breast tissue or see it.
An estimated 40 percent of women have dense breast tissue that may mask the presence of cancerous tissue in standard mammography. Dense breast tissue decreases with age, but remains important throughout life. Over 75 percent of women in their 40s have dense breast tissue but over a third of women in their 70s have dense breast tissue.
As breast density increases, mammography sensitivity decreases. This is significant, but we must consider the increased risk of breast cancer in women with dense breast tissue. Women with dense breast tissue have up to a four-fold increased risk of developing breast cancer. So, breast density is essentially the “perfect storm” where the ability to detect cancer decreases while the risk for breast cancer increases. Therefore, optimal approaches to individualized breast cancer screening are needed.
 Dr. Taylor-Phillips[/caption]
Dr Sian Taylor-Phillips PhD
Assistant Professor of Screening and Test Evaluation
Division of Health Sciences
Warwick Medical School
University of Warwick
Coventry
MedicalResearch.com: What is the background for this study?
Dr Taylor-Phillips : Psychologists have been investigating a phenomenon of a drop in performance with time on a task called ‘the vigilance decrement’ since World War 2. In those days radar operators searched for enemy aircraft and submarines (appearing as little dots of light on a radar screen). People thought that the ability to spot the dots might go down after too much time spent on the task. Many psychology experiments have found a vigilance decrement, but most of this research has not been in a real world setting.
In this research we wanted to know whether there was a drop in performance with time on a task for breast screening readers looking at breast x-rays for signs of cancer. (Breast x-rays or mammograms show lots of overlapping tissue and cancers can be quite difficult to spot). This was a real-world randomised controlled study in UK clinical practice.
In the UK NHS Breast Screening Programme two readers examine each woman’s breast x-rays separately for signs of cancer. They look at batches of around 35 women’s x-rays. At the moment both readers look at the x-rays in the same order as each another, so if they both experience a drop in performance, it will happen at the same time. We tested a really simple idea of reversing the batch order for one of the readers, so that if they have a low ebb of performance it happens when they are looking at different women’s breast x-rays.
Dr. Taylor-Phillips[/caption]
Dr Sian Taylor-Phillips PhD
Assistant Professor of Screening and Test Evaluation
Division of Health Sciences
Warwick Medical School
University of Warwick
Coventry
MedicalResearch.com: What is the background for this study?
Dr Taylor-Phillips : Psychologists have been investigating a phenomenon of a drop in performance with time on a task called ‘the vigilance decrement’ since World War 2. In those days radar operators searched for enemy aircraft and submarines (appearing as little dots of light on a radar screen). People thought that the ability to spot the dots might go down after too much time spent on the task. Many psychology experiments have found a vigilance decrement, but most of this research has not been in a real world setting.
In this research we wanted to know whether there was a drop in performance with time on a task for breast screening readers looking at breast x-rays for signs of cancer. (Breast x-rays or mammograms show lots of overlapping tissue and cancers can be quite difficult to spot). This was a real-world randomised controlled study in UK clinical practice.
In the UK NHS Breast Screening Programme two readers examine each woman’s breast x-rays separately for signs of cancer. They look at batches of around 35 women’s x-rays. At the moment both readers look at the x-rays in the same order as each another, so if they both experience a drop in performance, it will happen at the same time. We tested a really simple idea of reversing the batch order for one of the readers, so that if they have a low ebb of performance it happens when they are looking at different women’s breast x-rays.
 Dr. Boolbol[/caption]
MedicalResearch.com Interview with:
Susan K. Boolbol, MD, FACS
Chief, Division of Breast Surgery
Chief, Appel-Venet Comprehensive Breast Service
Co-Director, Breast Surgery Fellowship
Mount Sinai Beth Israel
Associate Professor of Surgery
Icahn School of Medicine at Mount Sinai
New York, NY 10003
Medical Research: What is the background for these new recommendations?
Dr. Boolbol: To make this final recommendation, the Task Force conducted a comprehensive review of the science since its 2009 recommendation and considered the public comments it received on its 2015 draft recommendation statement. Based on all of this, the task force issued their recommendations.
Medical Research: What are the main changes from current guidelines?
Dr. Boolbol: Presently, there are several different guidelines and recommendations regarding screening mammography. Depending on the group issuing the guidelines, the recommendations vary from annual mammography beginning at 40 years old to biennial mammograms from 50 to 74 years old. The Task Force continues to find that the benefit of mammography increases with age, and recommends biennial screening in women ages 50 to 74.
Dr. Boolbol[/caption]
MedicalResearch.com Interview with:
Susan K. Boolbol, MD, FACS
Chief, Division of Breast Surgery
Chief, Appel-Venet Comprehensive Breast Service
Co-Director, Breast Surgery Fellowship
Mount Sinai Beth Israel
Associate Professor of Surgery
Icahn School of Medicine at Mount Sinai
New York, NY 10003
Medical Research: What is the background for these new recommendations?
Dr. Boolbol: To make this final recommendation, the Task Force conducted a comprehensive review of the science since its 2009 recommendation and considered the public comments it received on its 2015 draft recommendation statement. Based on all of this, the task force issued their recommendations.
Medical Research: What are the main changes from current guidelines?
Dr. Boolbol: Presently, there are several different guidelines and recommendations regarding screening mammography. Depending on the group issuing the guidelines, the recommendations vary from annual mammography beginning at 40 years old to biennial mammograms from 50 to 74 years old. The Task Force continues to find that the benefit of mammography increases with age, and recommends biennial screening in women ages 50 to 74.
 Prof. Hennekens[/caption]
MedicalResearch.com Interview with:
Professor Charles Hennekens MD Dr.P.H
Sir Richard Doll Professor
Senior Academic Advisor to the Dean
Charles E. Schmidt College of Medicine
Florida Atlantic University
777 Glades Road
Boca Raton, FL 33431
Medical Research: What is the background for this study? What are the main findings?
Prof. Hennekens: Randomized evidence indicates clear benefits of mammography in middle age and, at present, most guidelines recommend regular mammography for women up to age 74. In collaboration with colleagues at Baylor Medical College and Meharry Medical School we were able to link the Surveillance, Epidemiology, and End Results (SEER) data to the Medicare administrative claims data. We found that, up to 84 years, screening was more common among whites than blacks and women receiving regular annual screening mammography had lower risks of mortality from breast cancer.
Prof. Hennekens[/caption]
MedicalResearch.com Interview with:
Professor Charles Hennekens MD Dr.P.H
Sir Richard Doll Professor
Senior Academic Advisor to the Dean
Charles E. Schmidt College of Medicine
Florida Atlantic University
777 Glades Road
Boca Raton, FL 33431
Medical Research: What is the background for this study? What are the main findings?
Prof. Hennekens: Randomized evidence indicates clear benefits of mammography in middle age and, at present, most guidelines recommend regular mammography for women up to age 74. In collaboration with colleagues at Baylor Medical College and Meharry Medical School we were able to link the Surveillance, Epidemiology, and End Results (SEER) data to the Medicare administrative claims data. We found that, up to 84 years, screening was more common among whites than blacks and women receiving regular annual screening mammography had lower risks of mortality from breast cancer.
 MedicalResearch.com Interview with:
Brian L. Sprague, PhD
Office of Health Promotion Research,
University of Vermont, Burlington, VT
MedicalResearch: What is the background for this study?
Dr. Sprague: Mammographic breast density refers to the appearance of breast tissue on a mammogram. High breast density means that there is a greater amount of glandular tissue and connective tissue, which appears white on a mammogram. It is more difficult to detect breast cancer on a mammogram when there is greater breast density. It has also been shown that women with dense breasts are at a higher risk of developing breast cancer. Because of these two factors, women with dense breasts have a greater chance of developing breast cancer after a normal screening mammogram than women whose breasts are not dense. Many states have now passed laws that require mammography facilities to inform women with dense breasts so that they are aware of this. Similar legislation is now under consideration at the national level. More than 40% of women undergoing mammography screening have dense breasts.
Researchers are trying to determine whether supplemental breast cancer screening with other tools would improve outcomes for women with dense breasts. One possible approach is to use ultrasound imaging to screen for breast cancer in women with dense breasts after they have had a normal mammogram. We wanted to estimate the benefits, harms, and cost-effectiveness of this approach compared to mammography screening only. No randomized trials or observational studies have assessed long term outcomes after ultrasound screening for women with dense breasts, but we have short term data on how often cancer is diagnosed by ultrasound screening and how often false positive exams occur. We used computer simulation modeling to estimate long term outcomes by combining the currently available data on mammography and ultrasound screening with the best available data on breast cancer risk and survival.
MedicalResearch.com Interview with:
Brian L. Sprague, PhD
Office of Health Promotion Research,
University of Vermont, Burlington, VT
MedicalResearch: What is the background for this study?
Dr. Sprague: Mammographic breast density refers to the appearance of breast tissue on a mammogram. High breast density means that there is a greater amount of glandular tissue and connective tissue, which appears white on a mammogram. It is more difficult to detect breast cancer on a mammogram when there is greater breast density. It has also been shown that women with dense breasts are at a higher risk of developing breast cancer. Because of these two factors, women with dense breasts have a greater chance of developing breast cancer after a normal screening mammogram than women whose breasts are not dense. Many states have now passed laws that require mammography facilities to inform women with dense breasts so that they are aware of this. Similar legislation is now under consideration at the national level. More than 40% of women undergoing mammography screening have dense breasts.
Researchers are trying to determine whether supplemental breast cancer screening with other tools would improve outcomes for women with dense breasts. One possible approach is to use ultrasound imaging to screen for breast cancer in women with dense breasts after they have had a normal mammogram. We wanted to estimate the benefits, harms, and cost-effectiveness of this approach compared to mammography screening only. No randomized trials or observational studies have assessed long term outcomes after ultrasound screening for women with dense breasts, but we have short term data on how often cancer is diagnosed by ultrasound screening and how often false positive exams occur. We used computer simulation modeling to estimate long term outcomes by combining the currently available data on mammography and ultrasound screening with the best available data on breast cancer risk and survival.
 MedicalResearch.com Interview with:
Elissa R. Price, MD
Assistant Professor of Clinical Radiology
Director of Clinical Operations, Breast Imaging
Breast Imaging Fellowship Program Director
Department of Radiology and Biomedical Imaging
University of California, San Francisco San Francisco, CA 94115
MedicalResearch: What is the background for this study? What are the main findings?
Dr. Price: Screening mammography recommendations for the 40 - 49 age group is very controversial. 2009 USPTF guidelines emphasized taking patient context into account when making decisions for these young women. Recent publications have suggested risk-based screening strategies. Family history and breast density are important are easily accessible risk factors.
Had we been using this risk-based approach to screening mammography at our institution, we would have missed more than 3Ž4 of the screen detected breast cancers in the 40-49 age group, thereby foregoing most of the survival benefit from screening mammography.
MedicalResearch.com Interview with:
Elissa R. Price, MD
Assistant Professor of Clinical Radiology
Director of Clinical Operations, Breast Imaging
Breast Imaging Fellowship Program Director
Department of Radiology and Biomedical Imaging
University of California, San Francisco San Francisco, CA 94115
MedicalResearch: What is the background for this study? What are the main findings?
Dr. Price: Screening mammography recommendations for the 40 - 49 age group is very controversial. 2009 USPTF guidelines emphasized taking patient context into account when making decisions for these young women. Recent publications have suggested risk-based screening strategies. Family history and breast density are important are easily accessible risk factors.
Had we been using this risk-based approach to screening mammography at our institution, we would have missed more than 3Ž4 of the screen detected breast cancers in the 40-49 age group, thereby foregoing most of the survival benefit from screening mammography.
 MedicalResearch.com Interview with:
Blake Cady MD
Professor of Surgery (emeritus) at Harvard Medical School
Partners HealthCare, Harvard Medical
School institutions, Boston
Medical Research: What are the main findings of this study?
Dr. Cady: Our findings support mammography screening, and our data is consistent
with the randomized trials. Breast cancer screening with mammography is the most extensively researched screening method ever studied. Only one “randomized" trial failed to show reduced mortality, (Canadian NCSS studies), and there were major flaws in its design and execution that negate their results, as noted in multiple critical publications (volunteers, not geographic assignment, palpable masses detected at examination assigned to “screening” arm, large contamination bias (control group got screened anyway), and very poor quality of mammography). Yet it is this NCSS study that is cited by critics and the press. “Failure Analyses” look backward from death, rather than forward from assignment in randomized trials. The concept of failure studies is well established as noted in recent reports of air-bag failures in cars, and many industrial studies. Seat belt prevention of deaths was discovered by police recording injuries and deaths in crashes after the fact - a failure analysis - not by randomized clinical trials. In breast cancer, failure analyses have advantages of little cost, early results, simplicity, and convenience, compared to randomized trials. Since our results support findings from randomized clinical trials (RCT), they can be accepted as reliable and accurate.
Our findings show that about 71% of deaths from breast cancer occur in the approximately 20% of our patients not in regular screening programs, while only 29% of deaths occur in the 80% of women who were regularly screened by mammography. By extrapolation, women regularly screened have only about a 5% breast cancer mortality, but women not screened have close to a 50% mortality.
(This is my extrapolation from our data, not direct data from our “Failure Analysis”)
MedicalResearch.com Interview with:
Blake Cady MD
Professor of Surgery (emeritus) at Harvard Medical School
Partners HealthCare, Harvard Medical
School institutions, Boston
Medical Research: What are the main findings of this study?
Dr. Cady: Our findings support mammography screening, and our data is consistent
with the randomized trials. Breast cancer screening with mammography is the most extensively researched screening method ever studied. Only one “randomized" trial failed to show reduced mortality, (Canadian NCSS studies), and there were major flaws in its design and execution that negate their results, as noted in multiple critical publications (volunteers, not geographic assignment, palpable masses detected at examination assigned to “screening” arm, large contamination bias (control group got screened anyway), and very poor quality of mammography). Yet it is this NCSS study that is cited by critics and the press. “Failure Analyses” look backward from death, rather than forward from assignment in randomized trials. The concept of failure studies is well established as noted in recent reports of air-bag failures in cars, and many industrial studies. Seat belt prevention of deaths was discovered by police recording injuries and deaths in crashes after the fact - a failure analysis - not by randomized clinical trials. In breast cancer, failure analyses have advantages of little cost, early results, simplicity, and convenience, compared to randomized trials. Since our results support findings from randomized clinical trials (RCT), they can be accepted as reliable and accurate.
Our findings show that about 71% of deaths from breast cancer occur in the approximately 20% of our patients not in regular screening programs, while only 29% of deaths occur in the 80% of women who were regularly screened by mammography. By extrapolation, women regularly screened have only about a 5% breast cancer mortality, but women not screened have close to a 50% mortality.
(This is my extrapolation from our data, not direct data from our “Failure Analysis”)
 MedicalResearch.com Interview with:
Anthony Miller, MD
Director, Canadian National Breast Screening Study
Professor Emeritus, Dalla Lana School of Public Health
University of Toronto
MedicalResearch.com: What are the main findings of the study?
Prof. Miller: The study involved 89,835 women aged 40 to 59. All underwent an annual physical breast examination, while half were randomly assigned to undergo annual mammograms for five years, beginning in 1980.
During the five-year screening period, 666 invasive breast cancers were diagnosed in the mammography arm and 524 in the controls. Over the 25 year follow-up 180 women in the mammography arm and 171 women in the control arm died of breast cancer. The overall hazard ratio for death from breast cancer diagnosed during the screening period associated with mammography was 1.05 (95% CI: 0.85 – 1.30). The findings for women aged 40-49 and aged 50-59 were almost identical.
After 15 years of follow-up an excess of 106 cancers was observed in the mammography arm, attributable to over-diagnosis, i.e. 22% of screen-detected invasive breast cancers, half of those detected by mammography alone. This represents one over-diagnosed breast cancer for every 424 women screened by mammography.
By 2005, 3,250 of the 44,925 women in the mammography arm of the study were diagnosed with breast cancer, and 500 had died of it. The control group of 44,910 women had 3,133 breast cancer diagnoses and 505 breast cancer deaths.
We conclude that annual mammography in women aged 40-59 does not reduce mortality from breast cancer beyond that of physical examination or usual care when adjuvant therapy for breast cancer is freely available.
MedicalResearch.com Interview with:
Anthony Miller, MD
Director, Canadian National Breast Screening Study
Professor Emeritus, Dalla Lana School of Public Health
University of Toronto
MedicalResearch.com: What are the main findings of the study?
Prof. Miller: The study involved 89,835 women aged 40 to 59. All underwent an annual physical breast examination, while half were randomly assigned to undergo annual mammograms for five years, beginning in 1980.
During the five-year screening period, 666 invasive breast cancers were diagnosed in the mammography arm and 524 in the controls. Over the 25 year follow-up 180 women in the mammography arm and 171 women in the control arm died of breast cancer. The overall hazard ratio for death from breast cancer diagnosed during the screening period associated with mammography was 1.05 (95% CI: 0.85 – 1.30). The findings for women aged 40-49 and aged 50-59 were almost identical.
After 15 years of follow-up an excess of 106 cancers was observed in the mammography arm, attributable to over-diagnosis, i.e. 22% of screen-detected invasive breast cancers, half of those detected by mammography alone. This represents one over-diagnosed breast cancer for every 424 women screened by mammography.
By 2005, 3,250 of the 44,925 women in the mammography arm of the study were diagnosed with breast cancer, and 500 had died of it. The control group of 44,910 women had 3,133 breast cancer diagnoses and 505 breast cancer deaths.
We conclude that annual mammography in women aged 40-59 does not reduce mortality from breast cancer beyond that of physical examination or usual care when adjuvant therapy for breast cancer is freely available.