Medicalresearch.com Interview with:
Dr. Pedro Recabal, MD and
Memorial Sloan Kettering Cancer Center Department of Surgery,
Urology Service New York, NY
Urology service, Fundacion Arturo Lopez Perez, Santiago, Chile
Dr. Vincent P. Laudone,
Memorial Sloan Kettering Cancer Center Department of Surgery
Urology Service New York, NY
Medicalresearch.com What is the background for this study?
Response: One of the most concerning adverse events that may arise following surgery for prostate cancer (radical prostatectomy) is postoperative erectile dysfunction. The loss of erectile function after surgery is most frequently caused by intraoperative injury to the neurovascular bundles, tiny packages of blood vessels and nerves that conduct the impulses responsible for erection. It is known that if both bundles are removed, patients seldom recover erectile function. Accordingly, neurovascular bundle preservation during Radical prostatectomy has proven benefits in terms of erectile function recovery.
However, as these bundles are intimately associated with the posterolateral aspects of the prostate, they must be carefully separated from the surface of the prostate without cutting them, applying excessive traction, or using cautery, all of which could produce irreversible damage and the consequent loss of function. During this dissection, the surgeon risks cutting into the prostatic capsule , which could result in leaving tumor behind. In some cases, the tumor extends beyond the prostate into the neurovascular bundles, and an attempt to preserve these structures could also result in incomplete tumor removal, defeating the purpose of radical prostatectomy.
Therefore, many urologists treating patients with “aggressive” tumors (such as the patients in our cohort) would try to avoid leaving cancer behind by removing not only the prostate but also the tissue around it, including the neurovascular bundles. In other words, if you had to chose between removing all the cancer but loosing erectile function, or preserving erectile function but risking an incomplete cancer removal, most patients and surgeons naturally lean towards the first option. Also, in many centers, patients with aggressive prostate cancers are managed with combined treatments (multimodal therapy), by adding hormonal therapy and/or radiotherapy, which could also result in erectile dysfunction. As such, many surgeons believe that there is no rationale for attempting to preserve the neurovascular bundles in these “high-risk” patients because most will end up with erectile dysfunction .
However, with the advent of MRI (and integrating other clinical information such as location of the positive biopsies, and intraoperative cues), surgeons can now have a better idea of where the cancer is located, which may aid in surgical planning. For instance, if a tumor is located in the anterior prostate, removing the neurovascular bundles (located on the posterolateral aspects) would provide no oncologic benefit, regardless of the aggressiveness of the tumor. Similarly, if the tumor compromises only the left side, removing the right neurovascular bundle is unlikely to help the patient, but can instead result in harm.
Moreover, neurovascular bundle preservation is not an all-or-none procedure; on each side, these bundles can be completely preserved (meaning dissecting exactly along the border between the prostate and the bundle); partially preserved (meaning preserving some of the nerves that are further away from the prostate, and removing the ones that are closer to the prostate); or completely removed along with the prostate (This has been graded in a scale from 1 to 4, where 1 represents complete preservation, and 4 represents complete removal of the neurovascular bundle, with 2 and 3 being partial preservation. This grade is recorded by the surgeon for each side, at the end of the procedure.) As such, sometimes it’s possible to preserve part of the bundle, even if there is a tumor on the same side
We designed a retrospective study to look at how high volume surgeons at MSKCC performed radical prostatectomy in high risk patients (how frequently and to what extent where the neurovascular bundles preserved), and what were the outcomes in terms of positive surgical margins (a surrogate for “leaving tumor behind”); use of additional oncologic treatments such as hormone therapy or radiotherapy, and finally, erectile function recovery in patients with functional erections before the operation. The patients in our cohort had at least one NCCN-defined high risk criteria (Gleason score ≥ 8; PSA ≥ 20 ng/ml; Clinical stage ≥ T3).














 Dr. Kenneth Iczkowski,[/caption]
Kenneth A. Iczkowski, M.D.
Department of Pathology
Medical College of Wisconsin
Milwaukee, WI 53226
MedicalResearch.com: What is the background for this study?
Dr. Iczkowski: The International Society of Urological Pathology (ISUP) in 2014 proposed use of a new 5-tier grade grouping system to supplement traditional Gleason grading to facilitate prognosis stratification and treatment1. The 5 categories subsume: Gleason 3+3=6, Gleason 3+4=7, Gleason 4+3=7, Gleason 8, and Gleason 9-10.
We desired to determine whether men with a highest Gleason score of 3+5=8 or 5+3=8 in their set of prostate biopsy specimens, would have differing outcomes from those with Gleason 4+4=8. Because Gleason 5 cancer has been demonstrated to have a higher biologic potential than Gleason 4, it was expected that Gleason score 8 pattern with any Gleason 5 pattern would have a worse outcome.
Dr. Kenneth Iczkowski,[/caption]
Kenneth A. Iczkowski, M.D.
Department of Pathology
Medical College of Wisconsin
Milwaukee, WI 53226
MedicalResearch.com: What is the background for this study?
Dr. Iczkowski: The International Society of Urological Pathology (ISUP) in 2014 proposed use of a new 5-tier grade grouping system to supplement traditional Gleason grading to facilitate prognosis stratification and treatment1. The 5 categories subsume: Gleason 3+3=6, Gleason 3+4=7, Gleason 4+3=7, Gleason 8, and Gleason 9-10.
We desired to determine whether men with a highest Gleason score of 3+5=8 or 5+3=8 in their set of prostate biopsy specimens, would have differing outcomes from those with Gleason 4+4=8. Because Gleason 5 cancer has been demonstrated to have a higher biologic potential than Gleason 4, it was expected that Gleason score 8 pattern with any Gleason 5 pattern would have a worse outcome.
 Dr. Kevin T. McVary[/caption]
Kevin T. McVary, MD, FACS
Chair, Division of Urology
The Pavilion at St. John’s Hospital
Springfield, IL
Chair and Professor of Urology
SIU School of Medicine
MedicalResearch.com: What is the background for this study? What are the main findings?
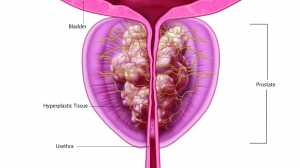
Dr. McVary: Benign Prostatic Hyperplasia (BPH) is a localized enlargement of the prostate gland in aging adult men. It affects approximately 75% of men over the age of 65. This excess growth of tissue compresses and obstructs the urethra, reducing the flow of urine from the bladder and sometimes blocking it entirely. As the symptoms increase, they can greatly impact a man’s quality of life. Both BPH and the existing treatments for it can negatively affect an individual’s sex life.
The Rezūm II IDE pivotal study was a prospective, multicenter, randomized (2:1) controlled trial that enrolled 197 patients across 15 clinical sites in the U.S. The main finding showed that radiofrequency generated convective water vapor thermal therapy provides rapid and sustainable improvement of lower urinary tract symptoms (LUTS) secondary to BPH and urinary flow over a 12-month period without negative effects on erectile and ejaculatory function. These results support the application of convective water vapor energy (WAVE) technology as safe and effective minimally invasive therapeutic alternative for symptomatic BPH. Additionally, no treatment or device related de novo erectile dysfunction occurred after thermal therapy, ejaculatory bother score improved 31% over baseline, and 27% of subjects achieved minimal clinically important differences (MCIDs) in erectile function scores at 1 year, including those with moderate to severe ED.
Dr. Kevin T. McVary[/caption]
Kevin T. McVary, MD, FACS
Chair, Division of Urology
The Pavilion at St. John’s Hospital
Springfield, IL
Chair and Professor of Urology
SIU School of Medicine
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. McVary: Benign Prostatic Hyperplasia (BPH) is a localized enlargement of the prostate gland in aging adult men. It affects approximately 75% of men over the age of 65. This excess growth of tissue compresses and obstructs the urethra, reducing the flow of urine from the bladder and sometimes blocking it entirely. As the symptoms increase, they can greatly impact a man’s quality of life. Both BPH and the existing treatments for it can negatively affect an individual’s sex life.
The Rezūm II IDE pivotal study was a prospective, multicenter, randomized (2:1) controlled trial that enrolled 197 patients across 15 clinical sites in the U.S. The main finding showed that radiofrequency generated convective water vapor thermal therapy provides rapid and sustainable improvement of lower urinary tract symptoms (LUTS) secondary to BPH and urinary flow over a 12-month period without negative effects on erectile and ejaculatory function. These results support the application of convective water vapor energy (WAVE) technology as safe and effective minimally invasive therapeutic alternative for symptomatic BPH. Additionally, no treatment or device related de novo erectile dysfunction occurred after thermal therapy, ejaculatory bother score improved 31% over baseline, and 27% of subjects achieved minimal clinically important differences (MCIDs) in erectile function scores at 1 year, including those with moderate to severe ED.


 Dr. R. Jeffrey Karnes[/caption]
MedicalResearch.com Interview with:
R. Jeffrey Karnes MD
Department of Urology, Mayo Clinic,
Rochester, MN 55905
MedicalResearch: What is the background for this study? What are the main findings?
Dr. Karnes: Cancer recurrence following radical prostatectomy is a concern for men undergoing definitive surgical treatment for prostate cancer. Approximately 20-35% of patients develop a rising prostate specific antigen following radical prostatectomy for clinically localized prostate cancer. PSA monitoring is an important tool for cancer surveillance; however, a standard PSA cutpoint to indicate biochemical recurrence has yet to be established. Over 60 different definitions have been described in literature. This variation creates confusion for the patients and clinicians. By studying a large group of patients who underwent radical prostatectomy at Mayo Clinic, we found that a PSA cutpoint of 0.4 ng/mL is the optimal definition for biochemical recurrence.
Dr. R. Jeffrey Karnes[/caption]
MedicalResearch.com Interview with:
R. Jeffrey Karnes MD
Department of Urology, Mayo Clinic,
Rochester, MN 55905
MedicalResearch: What is the background for this study? What are the main findings?
Dr. Karnes: Cancer recurrence following radical prostatectomy is a concern for men undergoing definitive surgical treatment for prostate cancer. Approximately 20-35% of patients develop a rising prostate specific antigen following radical prostatectomy for clinically localized prostate cancer. PSA monitoring is an important tool for cancer surveillance; however, a standard PSA cutpoint to indicate biochemical recurrence has yet to be established. Over 60 different definitions have been described in literature. This variation creates confusion for the patients and clinicians. By studying a large group of patients who underwent radical prostatectomy at Mayo Clinic, we found that a PSA cutpoint of 0.4 ng/mL is the optimal definition for biochemical recurrence.

