

25 Apr Researchers Found Why CBD Affects Anxiety Differently in Each Person
[caption id="attachment_73388" align="aligncenter" width="500"] SOURCE: IMAGE[/caption]
Editor's note: Cannabis and THCA/Hemp CBD products should have an active ingredient list on the container and a Certificate of Analysis (COA). Discuss your use of THC, cannabis, or CBD products with your health care provider. Dosing of cannabis products is variable, especially since they are not FDA regulated. Cannabis/CBD may interfere with other medications and should not be used in individuals with certain health conditions, including liver issues. CBD skin care products can be absorbed through the skin and have similar effects. Do not use cannabis products including edibles, drinks, and CBD if you are pregnant, nursing, or may become pregnant. Do not use cannabis products if driving or operating difficult or dangerous machinery. Children should not be exposed to cannabis or CBD products.
A question that comes up constantly in cannabis research is one that patients have been asking for years: why does CBD ease anxiety in one person and make another feel worse? For a long time, the honest answer was that nobody fully knew. A landmark study out of McGill University changedthat, and the findings reveal something that most consumer guides on CBD have never properly explained.
The answer is not about product quality, dosage form, or brand. It comes down to how cannabis interacts with serotonin — and specifically why that interaction is not the same at every dose.







 Elena Stains[/caption]
Elena Stains
Medical Student
Department of Medical Education
Geisinger Commonwealth School of Medicine
Scranton, PA
MedicalResearch.com: What is the background for this study?
Response: In 2019 to 2020, 2.5% of Americans reported using cannabis for medical needs, compared to 1.2% in 2013-2014, representing a 12.9% annual increase1. Forty states and the District of Columbia have legislation for some form of medical cannabis (MC) in 2024. Because MC is not federally legalized, each state creates its own legislation on the conditions that qualify a person for MC, without any standardized process to determine what qualifying conditions (QC) are proven to be aided by MC. Thus, the QCs chosen by states vary widely. Common QCs include cancer, dementia, and PTSD.
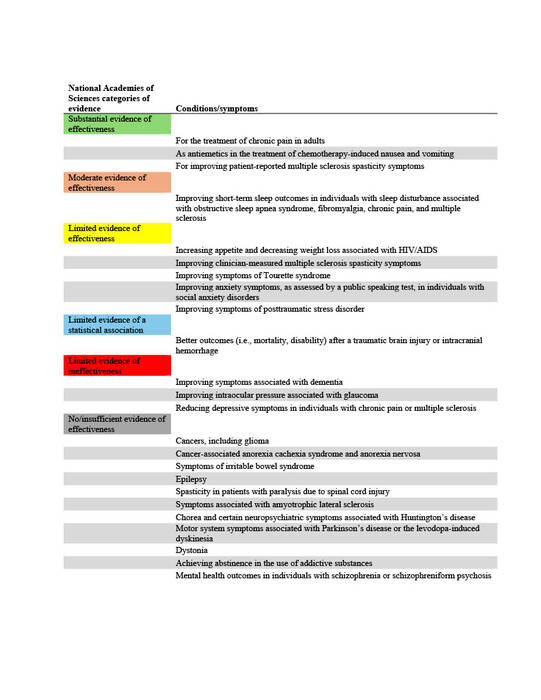
The National Academies of Sciences, Engineering, and Medicine (NAS) published a report in 2017 on the evidence for the therapeutic effects of cannabis and cannabinoids for over twenty conditions2. This report reviews the evidence of effectiveness of medical cannabis for the most common QCs chosen by states. The researchers at Geisinger Commonwealth School of Medicine aimed to compare the evidence found by the NAS report with the QCs of 38 states (including the District of Columbia) in both 2017 and 2024. QCs were categorized based on NAS-established level of evidence: limited, moderate, or substantial/conclusive evidence of effectiveness, limited evidence of ineffectiveness, or no/insufficient evidence to support or refute effectiveness (Table 1).
Elena Stains[/caption]
Elena Stains
Medical Student
Department of Medical Education
Geisinger Commonwealth School of Medicine
Scranton, PA
MedicalResearch.com: What is the background for this study?
Response: In 2019 to 2020, 2.5% of Americans reported using cannabis for medical needs, compared to 1.2% in 2013-2014, representing a 12.9% annual increase1. Forty states and the District of Columbia have legislation for some form of medical cannabis (MC) in 2024. Because MC is not federally legalized, each state creates its own legislation on the conditions that qualify a person for MC, without any standardized process to determine what qualifying conditions (QC) are proven to be aided by MC. Thus, the QCs chosen by states vary widely. Common QCs include cancer, dementia, and PTSD.
The National Academies of Sciences, Engineering, and Medicine (NAS) published a report in 2017 on the evidence for the therapeutic effects of cannabis and cannabinoids for over twenty conditions2. This report reviews the evidence of effectiveness of medical cannabis for the most common QCs chosen by states. The researchers at Geisinger Commonwealth School of Medicine aimed to compare the evidence found by the NAS report with the QCs of 38 states (including the District of Columbia) in both 2017 and 2024. QCs were categorized based on NAS-established level of evidence: limited, moderate, or substantial/conclusive evidence of effectiveness, limited evidence of ineffectiveness, or no/insufficient evidence to support or refute effectiveness (Table 1).












 Dr. Di Ciano[/caption]
Patricia Di Ciano, PhD
Dr. Di Ciano[/caption]
Patricia Di Ciano, PhD


 Luke Cavanah[/caption]
Luke Cavanah, BS
Geisinger Commonwealth School of Medicine
Scranton, PA
MedicalResearch.com: What is the background for this study?
Response: It is well-known that schedule II stimulants, which are those that are highly addictive and include amphetamine, methylphenidate, and lisdexamfetamine, have had increasing use and misuse in the US.
Despite understanding the presence of this phenomenon, the reason for it is poorly understood. The purpose of this study was to see if rising rates of schedule II stimulants are related to the legalization of medical marijuana. We were interested in this because schedule II stimulants are primarily used as the treatment for attention-deficit hyperactivity disorder (ADHD), chronic cannabis use has been demonstrated to cause neurocognitive deficits resembling that of ADHD, and the conditions have been shown to affect similar brain regions.
Luke Cavanah[/caption]
Luke Cavanah, BS
Geisinger Commonwealth School of Medicine
Scranton, PA
MedicalResearch.com: What is the background for this study?
Response: It is well-known that schedule II stimulants, which are those that are highly addictive and include amphetamine, methylphenidate, and lisdexamfetamine, have had increasing use and misuse in the US.
Despite understanding the presence of this phenomenon, the reason for it is poorly understood. The purpose of this study was to see if rising rates of schedule II stimulants are related to the legalization of medical marijuana. We were interested in this because schedule II stimulants are primarily used as the treatment for attention-deficit hyperactivity disorder (ADHD), chronic cannabis use has been demonstrated to cause neurocognitive deficits resembling that of ADHD, and the conditions have been shown to affect similar brain regions.

 Dr. Miller[/caption]
Alex P. Miller, PhD
TranSTAR T32 Postdoctoral Fellow
Department of Psychiatry
Washington University School of Medicine
St. Louis, MO
MedicalResearch.com: What is the background for this study?
Response: Adolescent cannabis use is increasing in the United States. Prior research suggests that people who start using cannabis earlier are more likely to engage in problematic use and also experience greater mental health challenges and socioeconomic disadvantages overall. For example, children who begin using cannabis early are more likely to have behavioral problems and disorders and are more less likely to complete school.
In our study, we used data from the Adolescent Brain Cognitive Development (ABCD) Study, which is following nearly 12,000 kids across the nation to track behavior and brain development as well as health from middle childhood to young adulthood. We looked at what factors are associated with the initiation of cannabis use by age 12-14.
Dr. Miller[/caption]
Alex P. Miller, PhD
TranSTAR T32 Postdoctoral Fellow
Department of Psychiatry
Washington University School of Medicine
St. Louis, MO
MedicalResearch.com: What is the background for this study?
Response: Adolescent cannabis use is increasing in the United States. Prior research suggests that people who start using cannabis earlier are more likely to engage in problematic use and also experience greater mental health challenges and socioeconomic disadvantages overall. For example, children who begin using cannabis early are more likely to have behavioral problems and disorders and are more less likely to complete school.
In our study, we used data from the Adolescent Brain Cognitive Development (ABCD) Study, which is following nearly 12,000 kids across the nation to track behavior and brain development as well as health from middle childhood to young adulthood. We looked at what factors are associated with the initiation of cannabis use by age 12-14.

 Dr. Lovestead[/caption]
Tara M Lovestead, PhD, (She/her/hers)
Dr. Lovestead[/caption]
Tara M Lovestead, PhD, (She/her/hers)
 Dr. Wong[/caption]
Mitchell Wong, MD PhD
Professor of Medicine
Executive Vice Chair for Research Training
Department of Medicine
Executive Co-Director, Specialty Training and Advanced Research (STAR) Program
Director, UCLA CTSI KL2 Program
UCLA Division of General Internal Medicine and Health Services Research Los Angeles, CA 90024
MedicalResearch.com: What is the background for this study?
Response: It is estimated that social factors like poverty, education, and housing have a large impact on health. Yet, there are few interventions that exist to directly address those issues. Schools are a promising solution since society already invests heavily in education and schools are an everyday part of most children’s lives.
Dr. Wong[/caption]
Mitchell Wong, MD PhD
Professor of Medicine
Executive Vice Chair for Research Training
Department of Medicine
Executive Co-Director, Specialty Training and Advanced Research (STAR) Program
Director, UCLA CTSI KL2 Program
UCLA Division of General Internal Medicine and Health Services Research Los Angeles, CA 90024
MedicalResearch.com: What is the background for this study?
Response: It is estimated that social factors like poverty, education, and housing have a large impact on health. Yet, there are few interventions that exist to directly address those issues. Schools are a promising solution since society already invests heavily in education and schools are an everyday part of most children’s lives.

 Sarah Windle[/caption]
Sarah Windle, MPH
PhD Student in Epidemiology
Department of Epidemiology, Biostatistics, and Occupational Health
McGill University (Montréal, Québec, Canada)
MedicalResearch.com: What is the background for this study?
Response: Concerns have been raised about the potential for increases in impaired driving following the legalization of recreational cannabis use in Canada in October 2018. Data from Statistics Canada suggest that cannabis use in the previous three months increased among adults (15 and older) from 14% before legalization in 2018 to 17% in 2019. Among those users with a driver’s license, 13% reported driving within two hours of cannabis use. While this proportion remained the same before and after legalization, this indicates that the absolute number of individuals who reported driving within two hours of use has increased following legalization (due to an increase in the number of users).
Sarah Windle[/caption]
Sarah Windle, MPH
PhD Student in Epidemiology
Department of Epidemiology, Biostatistics, and Occupational Health
McGill University (Montréal, Québec, Canada)
MedicalResearch.com: What is the background for this study?
Response: Concerns have been raised about the potential for increases in impaired driving following the legalization of recreational cannabis use in Canada in October 2018. Data from Statistics Canada suggest that cannabis use in the previous three months increased among adults (15 and older) from 14% before legalization in 2018 to 17% in 2019. Among those users with a driver’s license, 13% reported driving within two hours of cannabis use. While this proportion remained the same before and after legalization, this indicates that the absolute number of individuals who reported driving within two hours of use has increased following legalization (due to an increase in the number of users).

 Dr. Bunik[/caption]
Maya Bunik, MD, MPH | Professor, Pediatrics
Medical Director, Child Health Clinic, Primary Care | Breastfeeding Management Clinic
Adult and Child Consortium for Health Outcomes Research and Delivery Science (ACCORDS)
School of Medicine| University of Colorado Anschutz Medical Campus
Children's Hospital Colorado
MedicalResearch.com: What is the background for this study?
Response: Marijuana legalization has been increasing in the United States, with increasing consumption of marijuana products. Currently, the American Academy of Pediatrics (AAP), American College of Obstetricians and Gynecologists (ACOG) and Academy of Breastfeeding Medicine (ABM) do not recommend marijuana use during pregnancy or lactation due to concerning though limited data on the effects of perinatal marijuana exposure.
As there has been increasing prevalence of women using marijuana during pregnancy due to legalization and perceptions of safety, we sought to determine the duration of THC excretion in breast milk among women who had evidence of marijuana use at delivery and abstained post-partum.
Dr. Bunik[/caption]
Maya Bunik, MD, MPH | Professor, Pediatrics
Medical Director, Child Health Clinic, Primary Care | Breastfeeding Management Clinic
Adult and Child Consortium for Health Outcomes Research and Delivery Science (ACCORDS)
School of Medicine| University of Colorado Anschutz Medical Campus
Children's Hospital Colorado
MedicalResearch.com: What is the background for this study?
Response: Marijuana legalization has been increasing in the United States, with increasing consumption of marijuana products. Currently, the American Academy of Pediatrics (AAP), American College of Obstetricians and Gynecologists (ACOG) and Academy of Breastfeeding Medicine (ABM) do not recommend marijuana use during pregnancy or lactation due to concerning though limited data on the effects of perinatal marijuana exposure.
As there has been increasing prevalence of women using marijuana during pregnancy due to legalization and perceptions of safety, we sought to determine the duration of THC excretion in breast milk among women who had evidence of marijuana use at delivery and abstained post-partum.