MedicalResearch.com Interview with:
[caption id="attachment_53699" align="alignleft" width="160"]

Prof. Coleman[/caption]
Professor Carl Coleman, JD
Professor of Law
Seton Hall Law School
MedicalResearch.com: Do health care workers have an ethical and/or legal obligation to provide treatment during an infectious disease outbreak? Are there exceptions such as pregnancy, if the health care worker is her/himself immunocompromised or have young children at home?
Response: As a legal matter, health care workers can generally be required to fulfill pre-existing employment or contractual obligations during an infectious disease outbreak. For example, an emergency room nurse who refuses to come to work during a pandemic can be disciplined or fired; a physician who breaches a contractual obligation to provide on-call services during an outbreak can be held liable for damages. In addition to loss of employment and contractual damages, other potential consequences for failing to honor pre-existing commitments during a pandemic could include professional discipline for patient abandonment and, for physicians with on-call responsibilities in hospital emergency departments, civil fines under the federal Emergency Medical Treatment and Active Labor Act.
This does not mean that health care workers are obligated to show up for work during a pandemic regardless of the circumstances. For example, under the Americans with Disabilities Act, health care workers who are immunocompromised can ask for a "reasonable accommodation," such as the right to work remotely (if possible) or to take leave. Under the Family and Medical Leave Act, employers with more than 50 employees must give workers up to 12 weeks of unpaid time off to care for a seriously ill immediate family member. In addition, federal labor laws allow employees to refuse to work under "abnormally dangerous conditions," which might apply in situations where an employer fails to provide necessary protective equipment. However, assuming protective equipment is available, it is not clear that an outbreak itself would be considered "abnormally dangerous," particularly in fields like emergency medicine, where exposure to contagious disease is always a foreseeable risk.
In most states, health care workers without pre-existing employment or contractual obligations cannot be compelled to treat patients during a pandemic. However, a few states have laws that authorize public health authorities to require health care professionals to work during public health emergencies. I am not aware of any state that has invoked this authority so far.
As for ethical obligations, in 2004, the American Medical Association (AMA) declared that "individual physicians have an obligation to provide urgent medical care during disasters," and that "this ethical obligation holds even in the face of greater than usual risks to their own safety, health or life." Some academic ethicists have expressed similar views. Common justifications for this position are that physicians "assumed the risk" of exposure to infectious diseases when they voluntarily committed themselves to the healing professions; that a "social contract" requires physicians to assume risks in exchange for their social status and privileges; and that individuals who are uniquely capable of providing life-saving care have an obligation to do so.
However, I am not persuaded that all physicians -- let alone health care workers more generally -- have an ethical obligation to provide treatment when doing so involves significant risk. A willingness to accept risk is not a condition of obtaining a medical license, nor is it part of the oaths that students commonly take at medical school graduation. While I agree that physicians have ethical obligations to contribute to society, there are many ways they can fulfill these obligations without assuming personal health risks. And even assuming that individuals who are in a unique position to provide life-saving care should normally do so, we generally do not expect people to rescue others from danger at significant risk to themselves.




 Prof. Garnier[/caption]
Gil Garnier PhD
Director and Professor
Bioresource Processing Research Institute of Australia (BioPRIA)
PALS ARC Industry Transformation Research Hub
Department of Chemical Engineering
Monash University
MedicalResearch.com: What is the background for this study?
Response: We wanted to develop a test that would be:
1) Reliable and fast to perform,
2) Easy and fast to manufacture,
3) Easy and fast to distribute and be adopted by the Health care community.
We also wanted to capitalize on our vast expertise and experience from developing novel blood typing tests. Our strategy was to develop a serology COVID test using the current Gel card technology available in most hospital and blood laboratories throughout the world. Equipment and expertise are already available from point of care setting to high throughput/automated systems measuring 100-200 test/ h. Also, these cards are currently produced by many companies all over and these can be shipped all international.
Prof. Garnier[/caption]
Gil Garnier PhD
Director and Professor
Bioresource Processing Research Institute of Australia (BioPRIA)
PALS ARC Industry Transformation Research Hub
Department of Chemical Engineering
Monash University
MedicalResearch.com: What is the background for this study?
Response: We wanted to develop a test that would be:
1) Reliable and fast to perform,
2) Easy and fast to manufacture,
3) Easy and fast to distribute and be adopted by the Health care community.
We also wanted to capitalize on our vast expertise and experience from developing novel blood typing tests. Our strategy was to develop a serology COVID test using the current Gel card technology available in most hospital and blood laboratories throughout the world. Equipment and expertise are already available from point of care setting to high throughput/automated systems measuring 100-200 test/ h. Also, these cards are currently produced by many companies all over and these can be shipped all international.


![MedicalResearch.com Interview with: Dr Herman Anne Service de Dermatologie Cliniques Universitaires Saint-Luc Avenue Hippocrate, 10 1200 Bruxelle MedicalResearch.com: What is the background for this study? Response: In the context of the COVID-19 pandemic, several cases of acro-located lesions (on foot or hands) suggestive of chilblains have been reported and were possibly related to COVID-19. We wanted to determine if chilblains, observed in many patients recently referred to our department, are indicative of COVID-19. MedicalResearch.com: Would you briefly explain what is meant by chilblains? Response: Chilblains are frequent cold induced inflammatory lesions. Chilblains are typically seen in winter and occur after repeated exposure to cold temperatures. Clinical presentation includes erythema and swelling on toes and/or digits followed by red-purple macules or patches. However, given the large number of patients affected, and the exceptionally high outdoor temperatures for the spring season over the past month and at the time of case-observation, cold-exposure seemed unlikely. These lesions were, therefore, suspected to be associated with COVID-19. However, to date, no study has proven a pathological link between these lesions and COVID-19. MedicalResearch.com: What are the main findings? Response: In our series of 31 patients who recently developed chilblains, negative nasopharyngeal swabs and the absence of anti-SARS-CoV-2 blood immunoglobulin (Ig)M and IgG antibodies in all patients included in your study suggested that these patients had not been infected with COVID-19. These lesions appeared not to be directly related to COVID-19. MedicalResearch.com: What should readers take away from your report? Response: One hypothesis points to an indirect consequence of the COVID-19 pandemic due to imposed community containment and lockdown measures. Indeed, all patients in this study had either been working from home or were home-schooled since the beginning of containment measures in Belgium (March 11, 2020) or were temporarily unemployed. As a result of containment measures, the majority (64.5%) of patients reported a decrease in their physical activity and significantly more time spent in sedentary positions in front of screens. Most of the patients declared that they remained barefoot or in socks most of the day. All these lifestyle changes can be considered as risk factors for developing chilblains. Therefore, it seems plausible that containment, through its collateral effects, may induce chilblains. Interestingly also, the mean BMI of the patients included was relatively low, suggesting that thin people may be more at risk of developing chilblains. MedicalResearch.com: What recommendations do you have for future research as a result of this work? Response: During the current pandemic, several reports have suggested a possible link between cutaneous manifestations including aural lesions such as chilblains, and COVID-19, however, only few patients were tested for SARS-CoV-2 by RT-PCR and no serologic tests were performed. Therefore, reliable testings (RT-PCR and serologic testing) are essential to confirm a potential association with COVID-19. Citation: Herman A, Peeters C, Verroken A, et al. Evaluation of Chilblains as a Manifestation of the COVID-19 Pandemic. JAMA Dermatol. Published online June 25, 2020. doi:10.1001/jamadermatol.2020.2368 https://jamanetwork.com/journals/jamadermatology/fullarticle/2767774 [subscribe] Last Modified: [last-modified] The information on MedicalResearch.com is provided for educational purposes only, and is in no way intended to diagnose, cure, or treat any medical or other condition. Always seek the advice of your physician or other qualified health and ask your doctor any questions you may have regarding a medical condition. In addition to all other limitations and disclaimers in this agreement, service provider and its third party providers disclaim any liability or loss in connection with the content provided on this website.](https://medicalresearch.com/wp-content/uploads/2020/06/chilblain-example-dermnet-nz.jpg)
![MedicalResearch.com Interview with: Sarah Messiah, PhD, MPH Professor of epidemiology, human genetics, and environmental sciences UTHealth School of Public Health Dallas MedicalResearch.com: What is the background for this study? Response: Given that obesity is a prevalent, serious, complex, chronic, and relapsing disease, and severe obesity is a deepening crisis, it is important to pay special attention to these challenges during the COVID-19 pandemic. This will avoid placing an even greater burden on individuals, health systems, and society in the post-COVID-19 recovery phase. Thus, it is critically important to document, in real time, how socioecological determinants of health are impacting behaviors among those with obesity. Before our study, how the COVID-19 pandemic is impacting weight management, health behaviors, and psychosocial health in particular among people with obesity was unknown. MedicalResearch.com: What are the main findings? Response: A total of 123 patients (87% female, mean age 51.2 years, mean BMI 40.2, 49.2% Non-Hispanic white, 28.7% Non-Hispanic black, 16.4% Hispanic, 7% other ethnicity, 33.1% completed bariatric surgery were included). -Two patients tested positive for SARS-CoV-2 and 14.6% reported symptoms. -10% lost their job since the beginning of the pandemic -25% reported food insecurity in that they sometimes, or always could not afford to eat balanced meals -72.8% reported increased anxiety and 83.6% increased depression since stay-at-home orders were initiated. -69.6% reported more difficultly in achieving weight loss goals -47.9% reported less exercise time and 55.8% reported less intensity -49.6% reported increased stockpiling of food -61.2% reported stress eating -61.2% reported following healthy diet plans more challenging - Hispanics were less likely to report anxiety versus non-Hispanic whites MedicalResearch.com: What should readers take away from your report? Response: In a relatively short period of time, our results show that there have been substantial perceptions in changes in health behaviors among patients with obesity. Our sample described a decreases in positive health behaviors, increases in deleterious behaviors and associated deterioration in mental health. Even though actual COVID-19 disease burden was low (1.7% tested positive for COVID-19 and another 14.6% reported symptoms), the pandemic is having a significant impact on those without infections. The major strength of this study is that it is the first snapshot into how the COVID-19 pandemic has influenced health behaviors for patients with obesity. Prior to the pandemic, it has been reported that Americans consume 20% of their calories from restaurants and that there are worsening disparities in fast food meal quality by race/ethnicity, education, and income. Due to recent economic challenges, patients may be more likely to select cheaper foods, which are often energy dense and nutrient poor. Therefore, even though we found more patients are cooking at home, the type of foods that are being stockpiled are likely to be processed foods due to their longer shelf life. These are associated with greater intake of fat, carbohydrate, and calories, which facilitate greater weight gain when compared to more balanced diets. It is possible Americans may be trading one pattern of low-quality consumption for another by choosing cheaper processed foods instead of eating out. MedicalResearch.com: What recommendations do you have for future research as a result of this work? Response: These results have implications for clinical practice and management of patients with obesity as we now move into post-COVID-19 relief efforts. Due to the increase in obesogenic behaviors related to the COVID-19 pandemic that were found here, it is paramount that healthcare access is not disrupted for patients with obesity. Maintaining these vital services will prevent exacerbating the negative health and economic consequences of excess body weight. This includes access to primary care providers, Obesity Medicine specialists and bariatric surgery programs. In addition to asking about diet and exercise patterns, screening for indicators of mental health, loneliness, financial stressors and behaviors that may influence body weight should be implemented by healthcare teams to combat this problem. Disclosures: This work was funded by the National Institutes of Health, National Institute on Minority Health and Health Disparities (Grant #R01MD011686). This work was a joint collaboration among investigators from UTHealth School of Public Health, UT Southwestern Medical Center and Minimally Invasive Surgical Associates. Citation: Almandoz, J.P., Xie, L., Schellinger, J.N., Mathew, M.S., Gazda, C., Ofori, A., Kukreja, S. and Messiah, S.E. (2020), Impact of COVID ‐19 Stay‐at‐Home Orders on Weight‐Related Behaviors Among Patients with Obesity. Clin Obes. Accepted Author Manuscript. doi:10.1111/cob.12386 [subscribe] [last-modified] The information on MedicalResearch.com is provided for educational purposes only, and is in no way intended to diagnose, cure, or treat any medical or other condition. Always seek the advice of your physician or other qualified health and ask your doctor any questions you may have regarding a medical condition. In addition to all other limitations and disclaimers in this agreement, service provider and its third party providers disclaim any liability or loss in connection with the content provided on this website.](https://medicalresearch.com/wp-content/uploads/2020/06/Dr-Sarah-E.-Messiah.jpg)





 Prof. Dagna[/caption]
Prof. Lorenzo Dagna MD FACP
Ospedale San Raffaele and
Vita-Salute San Raffaele University
Milan, Italy
MedicalResearch.com: What is the background for this study?
Response: Upon encountering pathogens, our immune system produces pro-inflammatory mediators, called cytokines. Cytokines activate cells from the immune system. In most people, production of cytokines is an appropriate and protective response to infection. However, some individuals develop excessive and detrimental inflammatory responses, which are even more harmful than the pathogen itself to the host organism.
We hypothesized that some patients with COVID-19 might develop excessive and detrimental inflammation, and that treatment with anti-inflammatory agents might be beneficial in this population.
Anakinra is an inhibitor of the pro-inflammatory molecule interleukin 1 (IL-1). It was originally marketed for the treatment of rheumatoid arthritis, but is now mostly used to treat a variety of pediatric inflammatory diseases.
Prof. Dagna[/caption]
Prof. Lorenzo Dagna MD FACP
Ospedale San Raffaele and
Vita-Salute San Raffaele University
Milan, Italy
MedicalResearch.com: What is the background for this study?
Response: Upon encountering pathogens, our immune system produces pro-inflammatory mediators, called cytokines. Cytokines activate cells from the immune system. In most people, production of cytokines is an appropriate and protective response to infection. However, some individuals develop excessive and detrimental inflammatory responses, which are even more harmful than the pathogen itself to the host organism.
We hypothesized that some patients with COVID-19 might develop excessive and detrimental inflammation, and that treatment with anti-inflammatory agents might be beneficial in this population.
Anakinra is an inhibitor of the pro-inflammatory molecule interleukin 1 (IL-1). It was originally marketed for the treatment of rheumatoid arthritis, but is now mostly used to treat a variety of pediatric inflammatory diseases. 


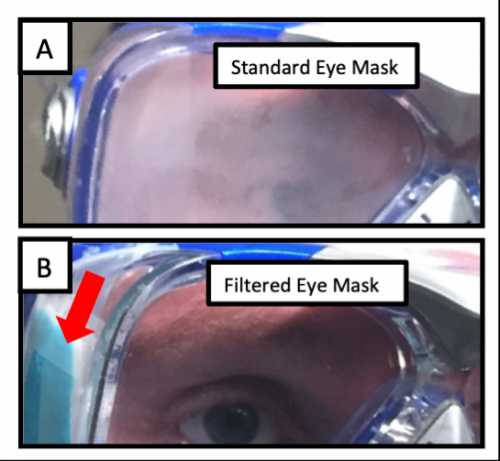

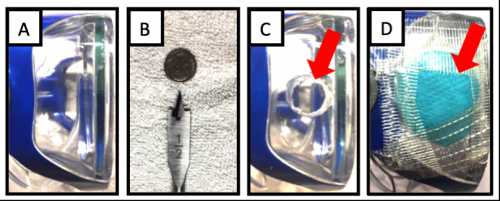 The building of the filtered eye mask prototype.[/caption]
The building of the filtered eye mask prototype.[/caption]




 Vasily Giannakeas[/caption]
Vasily Giannakeas, MPH
Epidemiologist/ Dedicated ICES Analyst
Women's College Hospital
Toronto, Ontario, Canada
MedicalResearch.com: What is the background for this study?
Response: As some health care systems approach collapse, a pressing need exists for tools modeling the capacity of acute and critical care systems during the COVID-19 pandemic.
We developed an online tool to estimate the maximum number of COVID-19 cases that could be managed per day within the catchment area served by a health care system, given acute and critical care resource availability.
The COVID-19 Acute and Intensive Care Resource Tool (CAIC-RT) is open access and available at
Vasily Giannakeas[/caption]
Vasily Giannakeas, MPH
Epidemiologist/ Dedicated ICES Analyst
Women's College Hospital
Toronto, Ontario, Canada
MedicalResearch.com: What is the background for this study?
Response: As some health care systems approach collapse, a pressing need exists for tools modeling the capacity of acute and critical care systems during the COVID-19 pandemic.
We developed an online tool to estimate the maximum number of COVID-19 cases that could be managed per day within the catchment area served by a health care system, given acute and critical care resource availability.
The COVID-19 Acute and Intensive Care Resource Tool (CAIC-RT) is open access and available at