MedicalResearch.com Interview with:
Craig A Umscheid, MD, MSCE, FACP
MedicalResearch.com Interview with:
Craig A Umscheid, MD, MSCE, FACP
Assistant Professor of Medicine and Epidemiology
Director, Center for Evidence-based Practice
Medical Director, Clinical Decision Support
Chair, Department of Medicine Quality Committee
Senior Associate Director, ECRI-Penn AHRQ Evidence-based Practice Center, University of Pennsylvania Philadelphia, PA 19104
Medical Research: What are the main findings of the study?
Dr. Umscheid: We developed an automated early warning and response system for sepsis that has resulted in a marked increase in sepsis identification and care, transfer to the ICU, and an indication of fewer deaths due to sepsis.
Sepsis is a potentially life-threatening complication of an infection; it can severely impair the body’s organs, causing them to fail. There are as many as three million cases of severe sepsis and 750,000 resulting deaths in the United States annually. Early detection and treatment, typically with antibiotics and intravenous fluids, is critical for survival.
The Penn prediction tool, dubbed the “sepsis sniffer,” uses laboratory and vital-sign data (such as body temperature, heart rate, and blood pressure) in the electronic health record of hospital inpatients to identify those at risk for
sepsis. When certain data thresholds are detected, the system automatically sends an electronic communication to physicians, nurses, and other members of a rapid response team who quickly perform a bedside evaluation and take action to stabilize or transfer the patient to the intensive care unit if warranted.
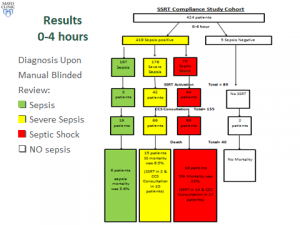
We developed the prediction tool using 4,575 patients admitted to the University of Pennsylvania Health System (UPHS) in October 2011. We then validated the tool during a pre-implementation period from June to September 2012, when data on admitted patients was evaluated and alerts triggered in a database, but no notifications were sent to providers on the ground. Outcomes in that control period were then compared to a post-implementation period from June to September 2013. The total number of patients included in the pre and post periods was 31,093.
(more…)