
Breast Cancer
14 Apr Infertility and Fertility Treatments Linked To Greater Breast Density
Posted at 20:48h
in Author Interviews, Breast Cancer, Fertility, Gender Differences, Karolinski Institute, Mammograms, Radiology
MedicalResearch.com Interview with:
[caption id="attachment_23484" align="alignleft" width="200"] Frida Lundberg[/caption]
Frida Lundberg | PhD Student
Dept. of Medical Epidemiology and Biostatistics
Karolinska Institutet
Medical Research: What is the background for this study?
Response: Fertility treatments involve stimulation with potent hormonal drugs that increase the amount of the sex hormones estrogen and progesterone. These hormones have been linked to breast cancer risk. Further, as these treatments are relatively new, most women who have gone through them are still below the age at which breast cancer is usually diagnosed. Therefore we wanted to investigate if infertility and fertility treatments influences mammographic breast density, a strong marker for breast cancer risk that is also hormone-responsive.
Medical Research: What are the main findings?
Response: We found that women with a history of infertility had higher absolute dense volume than other women. Among the infertile women, those who had gone through controlled ovarian stimulation (COS) had the highest absolute dense volume. The results from our study indicate that infertile women, especially those who undergo COS, might represent a group with an increased risk of breast cancer. However, the observed difference in dense volume was relatively small and has only been linked to a modest increase in breast cancer risk in previous studies. As the infertility type could influence what treatment the couples undergo, the association might also be due to the underlying infertility rather than the treatment per se.
Frida Lundberg[/caption]
Frida Lundberg | PhD Student
Dept. of Medical Epidemiology and Biostatistics
Karolinska Institutet
Medical Research: What is the background for this study?
Response: Fertility treatments involve stimulation with potent hormonal drugs that increase the amount of the sex hormones estrogen and progesterone. These hormones have been linked to breast cancer risk. Further, as these treatments are relatively new, most women who have gone through them are still below the age at which breast cancer is usually diagnosed. Therefore we wanted to investigate if infertility and fertility treatments influences mammographic breast density, a strong marker for breast cancer risk that is also hormone-responsive.
Medical Research: What are the main findings?
Response: We found that women with a history of infertility had higher absolute dense volume than other women. Among the infertile women, those who had gone through controlled ovarian stimulation (COS) had the highest absolute dense volume. The results from our study indicate that infertile women, especially those who undergo COS, might represent a group with an increased risk of breast cancer. However, the observed difference in dense volume was relatively small and has only been linked to a modest increase in breast cancer risk in previous studies. As the infertility type could influence what treatment the couples undergo, the association might also be due to the underlying infertility rather than the treatment per se.
14 Apr Acupuncture May Improved Hot Flashes in Breast Cancer Patients
MedicalResearch.com Interview with: Giorgia Razzini, PhD Unit of Medical Oncology Civil Hospital Carpi Italy; MedicalResearch.com: What is the background for this study? What are the main findings? Dr. Razzini: Hot flashes experienced by breast cancer patients is a significant clinical problem because there are few reliable treatment that are free of side effects and it sometime reduces compliance with endocrine therapy for prevention of cancer recurrence. Menopausal symtoms overall heavily impact on quality of life.. Acclimat found that acupuncture combined with self-care for 3 months, is associated with significantly lower hot flash scores, compared to self-care alone ( advices on diet, physical exercise and psycoloigical support if needed). Beneficial effects persisted up to 6 months follow-up. These effects were not associated with significant adverse events. MedicalResearch.com: What should clinicians and patients take away from your report? Dr. Razzini: Research suggests that breast cancer women do not receive adequate care for menopausal symptoms in the clinical practice of most oncology department. Our study showed that oncologists can offer them specific integrative management strategy for menopausal symptoms including acupuncture and enhanced self-care to women with breast cancer, particularly in younger women when treatment with hormonal treatment is recommended, in order to help women to stay on their therapy and improve their quality of life.08 Apr Adding Ovarian Suppression to Tamoxifen Worsens Menopausal Symptoms in Early Breast Cancer Patients
Posted at 21:26h
in Author Interviews, Breast Cancer, Endocrinology, Journal Clinical Oncology, Menopause
MedicalResearch.com Interview with:
[caption id="attachment_23339" align="alignleft" width="200"] Dr. Karin Ribi[/caption]
Karin Ribi, PhD, MPH
Head of Quality of Life Office
IBCSG
International Breast Cancer Study Group
Bern Switzerland
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Ribi: This study investigated the quality of life (QoL) outcomes for women in the Suppression of Ovarian Function (SOFT) trial. SOFT investigated the value of adding ovarian suppression (OFS) to tamoxifen and to determine the role of the aromatase inhibitor exemestane+OFS as adjuvant (post-surgery) therapies for hormone-sensitive early breast cancer. SOFT was conducted by the International Breast Cancer Study Group (IBCSG) in over 3000 premenopausal women from more than 500 centers worldwide. The primary analysis of SOFT compared tamoxifen alone with tamoxifen+OFS in over 2000 women, and showed that adding OFS to tamoxifen did not provide a significant benefit in the overall population of premenopausal women. However, for women who were at sufficient risk for recurrence to warrant adjuvant chemotherapy and who remained premenopausal, the addition of OFS improved disease outcomes.[1]
With regard to the QoL main findings, patients on tamoxifen+OFS were more affected than patients on tamoxifen alone by hot flushes at 6 and 24 months, by loss of sexual interest and sleep disturbance at 6 months, and by vaginal dryness up to 60 months. Without prior chemotherapy, patients on tamoxifen alone reported more vaginal discharge over the 5 years than patients on tamoxifen+OFS. Symptom-specific treatment differences at 6 months were less pronounced in patients with prior chemotherapy. Changes in global QoL indicators from baseline were small and similar between treatments over the whole treatment period.
Dr. Karin Ribi[/caption]
Karin Ribi, PhD, MPH
Head of Quality of Life Office
IBCSG
International Breast Cancer Study Group
Bern Switzerland
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Ribi: This study investigated the quality of life (QoL) outcomes for women in the Suppression of Ovarian Function (SOFT) trial. SOFT investigated the value of adding ovarian suppression (OFS) to tamoxifen and to determine the role of the aromatase inhibitor exemestane+OFS as adjuvant (post-surgery) therapies for hormone-sensitive early breast cancer. SOFT was conducted by the International Breast Cancer Study Group (IBCSG) in over 3000 premenopausal women from more than 500 centers worldwide. The primary analysis of SOFT compared tamoxifen alone with tamoxifen+OFS in over 2000 women, and showed that adding OFS to tamoxifen did not provide a significant benefit in the overall population of premenopausal women. However, for women who were at sufficient risk for recurrence to warrant adjuvant chemotherapy and who remained premenopausal, the addition of OFS improved disease outcomes.[1]
With regard to the QoL main findings, patients on tamoxifen+OFS were more affected than patients on tamoxifen alone by hot flushes at 6 and 24 months, by loss of sexual interest and sleep disturbance at 6 months, and by vaginal dryness up to 60 months. Without prior chemotherapy, patients on tamoxifen alone reported more vaginal discharge over the 5 years than patients on tamoxifen+OFS. Symptom-specific treatment differences at 6 months were less pronounced in patients with prior chemotherapy. Changes in global QoL indicators from baseline were small and similar between treatments over the whole treatment period.
05 Apr Shorter Overnight Fast May Increase Risk of Breast Cancer Recurrence
MedicalResearch.com Interview with: [caption id="attachment_23016" align="alignleft" width="130"] Dr. Ruth Patterson[/caption]
Ruth E. Patterson, PhD
Professor, Department of Family Medicine and Public Health
Associate Director, Population Sciences
Program Leader, Cancer Prevention
Moores Cancer Center
UC San Diego
La Jolla, CA
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Patterson: Our research team was intrigued with studies in mice showing that even when eating a high-fat diet, mice who were subjected to a 16-hour fasting regimen during the sleep phase were protected against abnormal glucose metabolism, inflammation and weight gain; all of which are associated with poor cancer outcomes.
We had access to a study conducted in breast cancer survivors called the Women’s Healthy Eating and Living Study (WHEL). Participants in this study completed food records, which give the time of eating meals and snacks. We used the food records to estimate the average nightly fasting interval in 2413 breast cancer survivors. Overall, we found that women who had a nightly fasting interval of less than 13 hours had a 36% increased risk of breast cancer recurrence and a nonsignificant increase in mortality. We also found that women with a short nightly fast had poorer glucoregulation and worse sleep, both of which might explain the link to breast cancer.
Dr. Ruth Patterson[/caption]
Ruth E. Patterson, PhD
Professor, Department of Family Medicine and Public Health
Associate Director, Population Sciences
Program Leader, Cancer Prevention
Moores Cancer Center
UC San Diego
La Jolla, CA
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Patterson: Our research team was intrigued with studies in mice showing that even when eating a high-fat diet, mice who were subjected to a 16-hour fasting regimen during the sleep phase were protected against abnormal glucose metabolism, inflammation and weight gain; all of which are associated with poor cancer outcomes.
We had access to a study conducted in breast cancer survivors called the Women’s Healthy Eating and Living Study (WHEL). Participants in this study completed food records, which give the time of eating meals and snacks. We used the food records to estimate the average nightly fasting interval in 2413 breast cancer survivors. Overall, we found that women who had a nightly fasting interval of less than 13 hours had a 36% increased risk of breast cancer recurrence and a nonsignificant increase in mortality. We also found that women with a short nightly fast had poorer glucoregulation and worse sleep, both of which might explain the link to breast cancer.
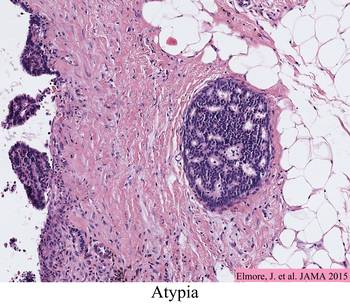
21 Mar Pathologists Often Disagree On Atypia or DCIS in Breast Biopsies
MedicalResearch.com Interview with: [caption id="attachment_22799" align="alignleft" width="161"] Dr. Joann Elmore[/caption]
Joann G. Elmore M.D., M.P.H.
Professor of Medicine,
Adjunct Professor of Epidemiology,
University of Washington School of Medicine
Harborview Medical Center
Seattle, WA 98104-2499
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Elmore: Our team began studying diagnostic agreement among pathologists while interpreting breast biopsies in 2009. Early findings from the Breast Pathology Study (B-Path) were published in March 2015 in the Journal of the American Medical Association and indicated strong agreement among pathologists when diagnosing invasive breast cancer or benign breast tissue. Agreement, however, was much lower for ductal carcinoma in situ (DCIS) and atypia. Results from this study raised concerns that a high percentage of breast biopsies may be inaccurately diagnosed. These concerns were amplified in the media with statements like “as many as one-in-four biopsies are incorrectly diagnosed.” Statements like this inaccurately depicted the results of our study, which included a test set weighted heavily with DCIS and atypia cases. It is important to consider the percentage that each outcome category contributes to the overall number of biopsies in the U.S. population as we found that the agreement rate of pathologists varies drastically across these diagnostic categories.
Dr. Joann Elmore[/caption]
Joann G. Elmore M.D., M.P.H.
Professor of Medicine,
Adjunct Professor of Epidemiology,
University of Washington School of Medicine
Harborview Medical Center
Seattle, WA 98104-2499
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Elmore: Our team began studying diagnostic agreement among pathologists while interpreting breast biopsies in 2009. Early findings from the Breast Pathology Study (B-Path) were published in March 2015 in the Journal of the American Medical Association and indicated strong agreement among pathologists when diagnosing invasive breast cancer or benign breast tissue. Agreement, however, was much lower for ductal carcinoma in situ (DCIS) and atypia. Results from this study raised concerns that a high percentage of breast biopsies may be inaccurately diagnosed. These concerns were amplified in the media with statements like “as many as one-in-four biopsies are incorrectly diagnosed.” Statements like this inaccurately depicted the results of our study, which included a test set weighted heavily with DCIS and atypia cases. It is important to consider the percentage that each outcome category contributes to the overall number of biopsies in the U.S. population as we found that the agreement rate of pathologists varies drastically across these diagnostic categories.
 In the new work published in Annals of Internal Medicine, we have analyzed the B-Path results to reflect variation among diagnoses of women using U.S. population-adjusted estimates,
In an effort to help physicians and patients better understand what the B-Path results mean for women, we have analyzed the B-Path results to reflect variation among diagnoses of women using U.S. population-adjusted estimates. When adjusted using population-based predictive value estimates, the B-Path results indicate that pathologists’ overall interpretations of breast biopsies would be confirmed by an expert panel 92 out of 100 biopsies, with more of the initial diagnoses over-interpreted rather than under-interpreted.
Of concern, our results noted that among 100 breast biopsies given an initial diagnosis of atypia, less than half of these cases would be given a diagnosis of atypia after review by a panel of three experienced breast pathologists. Over half of the biopsies would be downgraded from atypia to a diagnosis of benign without atypia after review.
In the new work published in Annals of Internal Medicine, we have analyzed the B-Path results to reflect variation among diagnoses of women using U.S. population-adjusted estimates,
In an effort to help physicians and patients better understand what the B-Path results mean for women, we have analyzed the B-Path results to reflect variation among diagnoses of women using U.S. population-adjusted estimates. When adjusted using population-based predictive value estimates, the B-Path results indicate that pathologists’ overall interpretations of breast biopsies would be confirmed by an expert panel 92 out of 100 biopsies, with more of the initial diagnoses over-interpreted rather than under-interpreted.
Of concern, our results noted that among 100 breast biopsies given an initial diagnosis of atypia, less than half of these cases would be given a diagnosis of atypia after review by a panel of three experienced breast pathologists. Over half of the biopsies would be downgraded from atypia to a diagnosis of benign without atypia after review.
20 Mar Biomarker of Mutant Stromal Cells May Detect Breast Cancer Early
MedicalResearch.com Interview with: [caption id="attachment_22795" align="alignleft" width="133"] Dr. Lan Ko[/caption]
Lan Ko MD PhD
Augusta University
Cancer Center
Augusta, GA 30912, USA
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Lan Ko: Cancer development hijacks normal cell differentiation. Understanding the normal is where we could begin to unlock the secret of cancer. In normal breast tissue, stem or progenitor cells produce supporting stromal cells in normal breast development. In breast cancer, the progenitor cells are mutated leaving mutant stromal cell offspring with altered activities to induce tumor. Mutant stem or progenitor cells may have longer lifespan than their mutant descendents so that they can fuel cancer growth for years. Eliminating those mutant progenitors at the source, at least in theory, will efficiently stop cancer.
Each subgroup of breast tumor stromal cells has been previously described by other scientists. However, the connections among these cells were unclear in the past. Like blind men feeling elephant, we scientists are often obscured from seeing the entire picture. The finding of mutant breast tumor stromal cells using GT198 as a marker provides a critical puzzle piece that fits the rest of puzzle together. When cancer problems can be viewed in multiple aspects with great simplicity, their connections emerge. We now know why breast cancer stromal cells are important, and how should we target them.
Dr. Lan Ko[/caption]
Lan Ko MD PhD
Augusta University
Cancer Center
Augusta, GA 30912, USA
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Lan Ko: Cancer development hijacks normal cell differentiation. Understanding the normal is where we could begin to unlock the secret of cancer. In normal breast tissue, stem or progenitor cells produce supporting stromal cells in normal breast development. In breast cancer, the progenitor cells are mutated leaving mutant stromal cell offspring with altered activities to induce tumor. Mutant stem or progenitor cells may have longer lifespan than their mutant descendents so that they can fuel cancer growth for years. Eliminating those mutant progenitors at the source, at least in theory, will efficiently stop cancer.
Each subgroup of breast tumor stromal cells has been previously described by other scientists. However, the connections among these cells were unclear in the past. Like blind men feeling elephant, we scientists are often obscured from seeing the entire picture. The finding of mutant breast tumor stromal cells using GT198 as a marker provides a critical puzzle piece that fits the rest of puzzle together. When cancer problems can be viewed in multiple aspects with great simplicity, their connections emerge. We now know why breast cancer stromal cells are important, and how should we target them.
18 Mar Arimidex and Tamoxifen Both Useful for Early Breast Cancer But with Different Safety Profiles
MedicalResearch.com Interview with: [caption id="attachment_22766" align="alignleft" width="136"] Prof. Jack Cuzick[/caption]
Professor Jack Cuzick, PhD, FMedSci, FRCP(hon)
Director, Wolfson Institute of Preventive Medicine and
Head, Centre for Cancer Prevention
Queen Mary University of London.
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Cuzick: Ductal carcinoma in situ (DCIS) is a very early form of breast cancer, where cancer cells are present in milk ducts, but have not spread to the surrounding breast tissue. It is estimated that approximately a fifth of all screen-detected breast cancers are DCIS, with around 4,800 people diagnosed with DCIS in the UK each year.
Our IBIS-II DCIS trial looked at 2,980 postmenopausal women with DCIS in 14 countries, who were either given anastrozole or tamoxifen for five years after surgery.
The two groups had a similar number of cases of the disease recurring, whether they took tamoxifen or anastrozole. Those who took anastrozole had an 11 per cent lower rate of recurrence of DCIS or invasive cancer than those who took tamoxifen, but this difference was not significant. The similar NSABP B-35 trial found a 29% reduction with anastrozole and the combined analysis of the two trials indicated a significant 21% reduction.
The key difference between the two groups were in the side effects of the medication. Women who took anastrozole experienced fewer womb and ovarian cancers and non melanoma skin cancers, and fewer deep vein thromboses and gynecological issues, compared with those who took tamoxifen. However more fractures and musculoskeletal side effects were seen among those receiving anastrozole.
Prof. Jack Cuzick[/caption]
Professor Jack Cuzick, PhD, FMedSci, FRCP(hon)
Director, Wolfson Institute of Preventive Medicine and
Head, Centre for Cancer Prevention
Queen Mary University of London.
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Cuzick: Ductal carcinoma in situ (DCIS) is a very early form of breast cancer, where cancer cells are present in milk ducts, but have not spread to the surrounding breast tissue. It is estimated that approximately a fifth of all screen-detected breast cancers are DCIS, with around 4,800 people diagnosed with DCIS in the UK each year.
Our IBIS-II DCIS trial looked at 2,980 postmenopausal women with DCIS in 14 countries, who were either given anastrozole or tamoxifen for five years after surgery.
The two groups had a similar number of cases of the disease recurring, whether they took tamoxifen or anastrozole. Those who took anastrozole had an 11 per cent lower rate of recurrence of DCIS or invasive cancer than those who took tamoxifen, but this difference was not significant. The similar NSABP B-35 trial found a 29% reduction with anastrozole and the combined analysis of the two trials indicated a significant 21% reduction.
The key difference between the two groups were in the side effects of the medication. Women who took anastrozole experienced fewer womb and ovarian cancers and non melanoma skin cancers, and fewer deep vein thromboses and gynecological issues, compared with those who took tamoxifen. However more fractures and musculoskeletal side effects were seen among those receiving anastrozole.
18 Mar Alcohol May Undo the Therapeutic Benefit of Tamoxifen in Breast Cancer
[caption id="attachment_22760" align="alignleft" width="133"] Dr. Chin Yo Lin[/caption]
MedicalResearch.com Interview with:
Chin-Yo Lin, Ph.D.
University of Houston
Center for Nuclear Receptors and Cell Signaling
Department of Biology and Biochemistry
Science and Engineering Research Center (SERC)
Houston, TX 77204-5056
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Lin: Many studies have established that alcohol consumption is a risk factor for breast cancer. Breast cancers associated with drinking tend to be hormone receptor-positive, the type is commonly treated with the drug tamoxifen which blocks the actions of estrogen in driving tumor growth in pre-menopausal women. Alcohol consumption has also been shown to increase the risk of disease recurrence in patients. Our study shows that alcohol can enhance the effects of estrogen by increasing cancer cell division and also reduce the efficacy of tamoxifen. The key mechanistic insight from the study is that alcohol treatment of breast cancer cells increased the expression of BRAF, a cancer-causing gene that is commonly mutated and activated in other types of cancers.
Dr. Chin Yo Lin[/caption]
MedicalResearch.com Interview with:
Chin-Yo Lin, Ph.D.
University of Houston
Center for Nuclear Receptors and Cell Signaling
Department of Biology and Biochemistry
Science and Engineering Research Center (SERC)
Houston, TX 77204-5056
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Lin: Many studies have established that alcohol consumption is a risk factor for breast cancer. Breast cancers associated with drinking tend to be hormone receptor-positive, the type is commonly treated with the drug tamoxifen which blocks the actions of estrogen in driving tumor growth in pre-menopausal women. Alcohol consumption has also been shown to increase the risk of disease recurrence in patients. Our study shows that alcohol can enhance the effects of estrogen by increasing cancer cell division and also reduce the efficacy of tamoxifen. The key mechanistic insight from the study is that alcohol treatment of breast cancer cells increased the expression of BRAF, a cancer-causing gene that is commonly mutated and activated in other types of cancers.
14 Mar Combination Treatment Causes Some HER2 Breast Cancers To Regress Quickly
MedicalResearch.com Interview with: [caption id="attachment_22492" align="alignleft" width="124"] Dr. Nigel Bundred[/caption]
Professor Nigel Bundred MD, FRCS
Professor of Surgical Oncology
Institute of Cancer Sciences
University Hospital of South Manchester
MedicalResearch.com: What is the background for this study?
Dr. Bundred: HER-2 is a cancer-causing gene which is expressed in some cells by having more copies of the gene and predicts for early relapse and metastasis from the tumour. Despite this, even in the absence of anything other than local treatment, some 50% of patients still survive for five years without relapse.
Herceptin was discovered and licensed for use in 2006 because it improved survival when given with chemotherapy after surgery, from 66% at five years to 90% at five years.
The use of Herceptin and chemotherapy before surgery to shrink the tumour indicates that around 30% of patients have a complete pathological response with this treatment.
Combination of dual anti-HER-2 therapies and Neoadjuvant chemotherapy given for six months before surgery has been shown to increase pCR rate to 50% and a single study utilising the combination of pertuzumab and trastuzumab (two anti-HER-2 monoclonal antibodies) given for four months revealed a 16.8% pCR rate.
Dr. Nigel Bundred[/caption]
Professor Nigel Bundred MD, FRCS
Professor of Surgical Oncology
Institute of Cancer Sciences
University Hospital of South Manchester
MedicalResearch.com: What is the background for this study?
Dr. Bundred: HER-2 is a cancer-causing gene which is expressed in some cells by having more copies of the gene and predicts for early relapse and metastasis from the tumour. Despite this, even in the absence of anything other than local treatment, some 50% of patients still survive for five years without relapse.
Herceptin was discovered and licensed for use in 2006 because it improved survival when given with chemotherapy after surgery, from 66% at five years to 90% at five years.
The use of Herceptin and chemotherapy before surgery to shrink the tumour indicates that around 30% of patients have a complete pathological response with this treatment.
Combination of dual anti-HER-2 therapies and Neoadjuvant chemotherapy given for six months before surgery has been shown to increase pCR rate to 50% and a single study utilising the combination of pertuzumab and trastuzumab (two anti-HER-2 monoclonal antibodies) given for four months revealed a 16.8% pCR rate.
09 Mar Treating Diabetes Can Reduce Breast Density on Mammograms
MedicalResearch.com Interview with: Dr. Zorana Andersen Department of Public Health Center for Epidemiology and Screening University of Copenhagen MedicalResearch.com: What is the background for this study? What are the main findings? Dr. Andersen: Diabetes is associated with increased risk of breast cancer, but exact mechanisms are unknown. The role of insulin has been debated. High mammographic density (MD) is one of the strongest predictors and a biomarker of breast cancer risk. Few studies have linked diabetes to mammographic density, finding none or weak inverse associations, but none had data on diabetes treatment. We examined whether diabetes and diabetes treatment are associated with mammographic density in a prospective cohort study of Danish women above age of 50 years. MedicalResearch.com: What should clinicians and patients take away from your report? Dr. Andersen: Women with diabetes, as well as clinicians working with diabetes and breast cancer and breast cancer screening, would have interest to know how different diabetes treatment can affect breast density, and hereby possibly breast cancer risk. For example, diabetic women taking insulin may possibly benefit from informing radiologists at breast cancer screening about their insulin use, due to increased breast density and increased risk of masking bias.09 Mar High Neutrophil to Lymphocyte Ratio Linked To Poor Prognosis in Early Breast Cancer
MedicalResearch.com Interview with: [caption id="attachment_22386" align="alignleft" width="150"] Dr. Michele Orditura[/caption]
Michele Orditura MD, PhD
Associate Professor in Medical Oncology
Faculty of Medicine, Second University of Naples
Naples Italy
MedicalResearch.com: What is the background for this study?
Prof. Orditura: In the last few years increasing evidence suggests that cancer-related inflammatory response plays a crucial role in the development and progression of several malignancies. Neutrophil to lymphocyte ratio (NLR), calculated as the neutrophil count divided by the lymphocyte count , may represent an easily measurable and inexpensive marker of systemic inflammation.
Several studies have reported NLR as an unfavourable prognostic indicator for patients with gastrointestinal, lung, renal and gynaecological cancers. In the breast cancer setting, the results of published trials evaluating the relationship between NLR and outcome are controversial, and a recent meta-analysis including eight trials published between 2012 and 2014 has shown that elevated NLR is strongly associated with poor survival. In addition, the available data mainly concern women of Asian race and only three papers have included patients of Europe race.
The main aim of this study was to clarify the correlation between pre surgery NLR and distant metastasis-free survival in a series of 300 Italian patients with early breast cancer. The propensity score-matched analysis was chosen for statistical evaluation to avoid risk of confounding bias.
Dr. Michele Orditura[/caption]
Michele Orditura MD, PhD
Associate Professor in Medical Oncology
Faculty of Medicine, Second University of Naples
Naples Italy
MedicalResearch.com: What is the background for this study?
Prof. Orditura: In the last few years increasing evidence suggests that cancer-related inflammatory response plays a crucial role in the development and progression of several malignancies. Neutrophil to lymphocyte ratio (NLR), calculated as the neutrophil count divided by the lymphocyte count , may represent an easily measurable and inexpensive marker of systemic inflammation.
Several studies have reported NLR as an unfavourable prognostic indicator for patients with gastrointestinal, lung, renal and gynaecological cancers. In the breast cancer setting, the results of published trials evaluating the relationship between NLR and outcome are controversial, and a recent meta-analysis including eight trials published between 2012 and 2014 has shown that elevated NLR is strongly associated with poor survival. In addition, the available data mainly concern women of Asian race and only three papers have included patients of Europe race.
The main aim of this study was to clarify the correlation between pre surgery NLR and distant metastasis-free survival in a series of 300 Italian patients with early breast cancer. The propensity score-matched analysis was chosen for statistical evaluation to avoid risk of confounding bias.
07 Mar Beta Blockers May Be Useful Adjuvant For Breast Cancer Through Stress Reduction
MedicalResearch.com Interview with: Michelle L. Halls BBiomedSci(Hons), PhD NHMRC Career Development Fellow Drug Discovery Biology Theme Monash Institute of Pharmaceutical Sciences Monash University Parkville Australia MedicalResearch.com: What is the background for this study? What are the main findings? Dr. Halls: Stress causes an increase in the release of hormones including adrenaline. Previous studies have found a link between stress and metastases in triple negative breast cancer. However, what occurs inside a cancer cell in response to adrenaline to drive cancer progression was not known. We have found that adrenaline can directly act on triple negative breast cancer tumour cells via a cell surface receptor called the beta2-adrenoceptor. We identified changes in signalling within the cell that make the tumour cell highly invasive by mapping the signalling pathways that were activated in these cells in response to stress. We found that different signalling pathways converge to amplify the final signal. This ‘positive signalling loop’ was linked to the increased invasion of these cells in response to stress, and was not identified in less aggressive breast cancer cells. This may allow future research to identify new ways to intervene and slow cancer progression. New therapies are important for triple negative breast cancer, as it is particularly aggressive and currently has limited treatment options.06 Mar Newly Identified Function of BRAC1 Suggests Target For Breast Cancer Prevention
MedicalResearch.com Interview with: [caption id="attachment_22440" align="alignleft" width="100"] Dr. Rong Li[/caption]
Rong Li, Ph.D., Professor
Holder of the Tom C. & H. Frost Endowment
Department of Molecular Medicine
Institute of Biotechnology
Co-Leader, Cancer Development and Progression Program
Cancer Therapy & Research Center
University of Texas Health Science Center at San Antonio
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Li: The breast cancer susceptibility gene BRCA1 is well known for its function in double strand break DNA repair. However, the ubiquitous role of BRCA1 in DNA repair may not be sufficient to explain its tissue-specific tumor suppressor function in vivo. Using the “awesome power” of mouse genetics, we identified a previously unappreciated crosstalk between BRCA1 and a transcription regulator in mammary gland development. Importantly, we provide compelling evidence that this BRCA1 function is independent of its well-established DNA repair activity.
MedicalResearch.com: What should clinicians and patients take away from your report?
Dr. Li: The newly identified DNA repair-independent function of BRCA1 may provide new tools and targets for early prevention of BRCA1-associated breast cancer.
Dr. Rong Li[/caption]
Rong Li, Ph.D., Professor
Holder of the Tom C. & H. Frost Endowment
Department of Molecular Medicine
Institute of Biotechnology
Co-Leader, Cancer Development and Progression Program
Cancer Therapy & Research Center
University of Texas Health Science Center at San Antonio
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Li: The breast cancer susceptibility gene BRCA1 is well known for its function in double strand break DNA repair. However, the ubiquitous role of BRCA1 in DNA repair may not be sufficient to explain its tissue-specific tumor suppressor function in vivo. Using the “awesome power” of mouse genetics, we identified a previously unappreciated crosstalk between BRCA1 and a transcription regulator in mammary gland development. Importantly, we provide compelling evidence that this BRCA1 function is independent of its well-established DNA repair activity.
MedicalResearch.com: What should clinicians and patients take away from your report?
Dr. Li: The newly identified DNA repair-independent function of BRCA1 may provide new tools and targets for early prevention of BRCA1-associated breast cancer.
04 Mar Patients May Benefit From New Combination Therapy For HER2-Negative Metastatic Breast Cancer
MedicalResearch.com Interview with: [caption id="attachment_22319" align="alignleft" width="200"] Dr. Massimo Cristofanilli[/caption]
Massimo Cristofanilli, MD, FACP
Professor of Medicine
Associate Director of Translational Research and Precision Medicine
Department of Medicine-Hematology and Oncology
Robert H Lurie Comprehensive Cancer Center
Feinberg School of Medicine
Chicago, IL 60611
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Cristofanilli: The majority of breast cancer are estrogen-receptor positive and therefore candidate for treatment with endocrine therapy in the adjuvant and advanced settings. The most significant issue in the management of estrogen-receptor positive metastatic breast cancer is the development of drug resistance. Very few effective options are available for patients that demonstrate progression of disease while on standard endocrine therapy, particularly in premenopausal women and/or women that have even progressed on chemotherapy. The study demonstrated that the combination of fulvestrant with palbociclib, a novel inhibitor of CDK4/6 kinases, significantly improve response to treatment and delays disease progression with minimal toxicity.
Dr. Massimo Cristofanilli[/caption]
Massimo Cristofanilli, MD, FACP
Professor of Medicine
Associate Director of Translational Research and Precision Medicine
Department of Medicine-Hematology and Oncology
Robert H Lurie Comprehensive Cancer Center
Feinberg School of Medicine
Chicago, IL 60611
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Cristofanilli: The majority of breast cancer are estrogen-receptor positive and therefore candidate for treatment with endocrine therapy in the adjuvant and advanced settings. The most significant issue in the management of estrogen-receptor positive metastatic breast cancer is the development of drug resistance. Very few effective options are available for patients that demonstrate progression of disease while on standard endocrine therapy, particularly in premenopausal women and/or women that have even progressed on chemotherapy. The study demonstrated that the combination of fulvestrant with palbociclib, a novel inhibitor of CDK4/6 kinases, significantly improve response to treatment and delays disease progression with minimal toxicity.
03 Mar Genetic Assay Oncotype Dx Helps Clarify Chemotherapy Decisions in HER2 Negative Breast Cancer
Posted at 12:18h
in ASCO, Author Interviews, Biomarkers, Breast Cancer, Chemotherapy, Genetic Research, Journal Clinical Oncology
MedicalResearch.com Interview with:
[caption id="attachment_22296" align="alignleft" width="200"] Dr. Oleg Gluz[/caption]
Oleg Gluz, MD
West German Study Group
Breast Center Niederrhein
Evangelical Hospital Bethesda
Moenchengladbach, Germany
MedicalResearch.com: What is the background for this study?
Dr. Gluz: PlanB trial is a Phase III chemotherapy study performed in patients with clinically high risk HER2 negative breast cancer. After early amendement, Recurrence Score (Oncotype Dx) as a selection criterion for or against chemotherapy together with central pathology review were included into the study. Patients with very low RS of below 12 and up to 3 positive lymph nodes were recommended to omit chemotherapy based on the low genomic recurrence risk. Chemotherapy was omitted in about 15% of all patients.
For the first time we present prospective data comparing a genomical tool (Oncotype Dx) and an independent central pathology review for grade, ER, PR, and Ki-67 from a large phase III study combined with an exploratory analysis on early relapse risk.
MedicalResearch.com: What are the main findings?
Dr. Gluz: The study has two major findings:
We have found a significant discordance in risk assessment between prognostic tools (grade by local and central lab, Oncotype Dx, Ki-67).
Patients treated by endocrine therapy alone based on very low Recurrence Score had an excellent disease free survival of 97% after 3 years of follow up.
Dr. Oleg Gluz[/caption]
Oleg Gluz, MD
West German Study Group
Breast Center Niederrhein
Evangelical Hospital Bethesda
Moenchengladbach, Germany
MedicalResearch.com: What is the background for this study?
Dr. Gluz: PlanB trial is a Phase III chemotherapy study performed in patients with clinically high risk HER2 negative breast cancer. After early amendement, Recurrence Score (Oncotype Dx) as a selection criterion for or against chemotherapy together with central pathology review were included into the study. Patients with very low RS of below 12 and up to 3 positive lymph nodes were recommended to omit chemotherapy based on the low genomic recurrence risk. Chemotherapy was omitted in about 15% of all patients.
For the first time we present prospective data comparing a genomical tool (Oncotype Dx) and an independent central pathology review for grade, ER, PR, and Ki-67 from a large phase III study combined with an exploratory analysis on early relapse risk.
MedicalResearch.com: What are the main findings?
Dr. Gluz: The study has two major findings:
We have found a significant discordance in risk assessment between prognostic tools (grade by local and central lab, Oncotype Dx, Ki-67).
Patients treated by endocrine therapy alone based on very low Recurrence Score had an excellent disease free survival of 97% after 3 years of follow up.
03 Mar Early Breast Cancer Screening Recommended For Survivors of Childhood Hodgkin’s Lymphoma
MedicalResearch.com Interview with: [caption id="attachment_22284" align="alignleft" width="200"] Dr. David Hodgson[/caption]
David Hodgson, MD, MPH, FRCPC
Associate Professor
University of Toronto
Toronto, ON Canada
MedicalResearch.com: What is the background for this study?
Dr. Hodgson: We know that treatment for childhood Hodgkin lymphoma can cause some side effects that arise years after treatment is finished. In particular, radiotherapy given to the chest of adolescent females increases the risk of developing breast cancer in young adult survivors. But there are very little data about whether the early initiation of breast cancer screening will prevent breast cancer deaths in these survivors, and what kinds of screening is optimal. This is important because less than half of these young survivors are undergoing breast cancer screening, and in some jurisdictions early screening is not covered by insurance.
MedicalResearch.com: What are the main findings?
Dr. Hodgson: Because there has not been, and likely never will be, a large randomized screening trial for these patients, we used all the available information about their breast cancer risk, other health issues and the effectiveness of screening, and created a mathematical model that allows us to estimate the number of breast cancer deaths prevented by starting screening at age 25 for women who had received chest RT as teenagers. We found that one would have to invite about 260 survivors to early mammographic screening to prevent one breast cancer death, which compares favorably to other accepted reasons for breast cancer screening. Using MRI for screening, approximately 80 women would have to be invited to prevent one breast cancer death, because MRI is so much more sensitive than mammography. One of the problems with MRI, however, is that a substantial number of women will have "false positive" tests - abnormal findings that are not really cancer.
Dr. David Hodgson[/caption]
David Hodgson, MD, MPH, FRCPC
Associate Professor
University of Toronto
Toronto, ON Canada
MedicalResearch.com: What is the background for this study?
Dr. Hodgson: We know that treatment for childhood Hodgkin lymphoma can cause some side effects that arise years after treatment is finished. In particular, radiotherapy given to the chest of adolescent females increases the risk of developing breast cancer in young adult survivors. But there are very little data about whether the early initiation of breast cancer screening will prevent breast cancer deaths in these survivors, and what kinds of screening is optimal. This is important because less than half of these young survivors are undergoing breast cancer screening, and in some jurisdictions early screening is not covered by insurance.
MedicalResearch.com: What are the main findings?
Dr. Hodgson: Because there has not been, and likely never will be, a large randomized screening trial for these patients, we used all the available information about their breast cancer risk, other health issues and the effectiveness of screening, and created a mathematical model that allows us to estimate the number of breast cancer deaths prevented by starting screening at age 25 for women who had received chest RT as teenagers. We found that one would have to invite about 260 survivors to early mammographic screening to prevent one breast cancer death, which compares favorably to other accepted reasons for breast cancer screening. Using MRI for screening, approximately 80 women would have to be invited to prevent one breast cancer death, because MRI is so much more sensitive than mammography. One of the problems with MRI, however, is that a substantial number of women will have "false positive" tests - abnormal findings that are not really cancer.
28 Feb Many Breast Cancer Patients Overestimate Risk of Recurrence and Spread
MedicalResearch.com Interview with: [caption id="attachment_22165" align="alignleft" width="133"] Dr. Sarah Hawley[/caption]
Sarah T. Hawley PhD MPH
Professor of Medicine
University of Michigan
Medical Research: What is the background for this study? What are the main findings?
Dr. Hawley: Research has shown that breast cancer patients do not have a good understanding of their risk of distant recurrence, and and that the fear of cancer spreading is one of the biggest concerns that patients have. The research that has been done shows that most patients over-esimate this risk, and think they have a bigger chance of the cancer coming back than they actually have. There has been relatively little done to investigate the association between patient over-estimation of risk and patient reported outcomes, specifically their quality of life. We therefore conducted our study to understand the extent of overestimation of risk in a population-based sample of breast cancer patients with very favorable prognosis (DCIS, low risk invasive breast cancer) using a numeric (number based) and descriptive (general understanding) measure, and to understand the association between over-estimation and quality of life.
The main findings are that almost 40% of our sample of patients over-estimated their risk; 33% using a numeric measure and 15% using a descriptive measure. There was no clear “type” of patient who overestimated her risk of distant recurrence, though women with lower education more over overestimated numerically than those with higher education.
Both numeric and descriptive over-estimation was associated with reduced quality of life outcomes, especially with frequency of worry about recurrence, however over estimating descriptively mattered the most. Women who overestimated their risk both numerically and descriptively had a nearly 10 fold odds of frequent worry compared to women who understood their risk.
Dr. Sarah Hawley[/caption]
Sarah T. Hawley PhD MPH
Professor of Medicine
University of Michigan
Medical Research: What is the background for this study? What are the main findings?
Dr. Hawley: Research has shown that breast cancer patients do not have a good understanding of their risk of distant recurrence, and and that the fear of cancer spreading is one of the biggest concerns that patients have. The research that has been done shows that most patients over-esimate this risk, and think they have a bigger chance of the cancer coming back than they actually have. There has been relatively little done to investigate the association between patient over-estimation of risk and patient reported outcomes, specifically their quality of life. We therefore conducted our study to understand the extent of overestimation of risk in a population-based sample of breast cancer patients with very favorable prognosis (DCIS, low risk invasive breast cancer) using a numeric (number based) and descriptive (general understanding) measure, and to understand the association between over-estimation and quality of life.
The main findings are that almost 40% of our sample of patients over-estimated their risk; 33% using a numeric measure and 15% using a descriptive measure. There was no clear “type” of patient who overestimated her risk of distant recurrence, though women with lower education more over overestimated numerically than those with higher education.
Both numeric and descriptive over-estimation was associated with reduced quality of life outcomes, especially with frequency of worry about recurrence, however over estimating descriptively mattered the most. Women who overestimated their risk both numerically and descriptively had a nearly 10 fold odds of frequent worry compared to women who understood their risk.
25 Feb More Young Women Getting BRCA Breast Cancer Genetic Testing
MedicalResearch.com Interview with: [caption id="attachment_22015" align="alignleft" width="175"] Dr. Shoshana Rosenberg[/caption]
Dr. Shoshana Rosenberg ScD, MPH
Department of Medical Oncology
Dana-Farber Cancer Institute
Boston, Massachusetts
Medical Research: Why would BRCA testing rates have increased among younger women with cancer?
Dr. Rosenberg: There has been increasing awareness surrounding genetic testing for breast cancer in more recent years, likely contributing to the trend that we saw over time in our cohort. This has included more media attention, most notably Angelina Jolie’s sharing her story in 2013.
Medical Research: Is this increase in testing a good thing?
Dr. Rosenberg: Young women who are diagnosed with breast cancer should be getting tested so the fact that an increasing proportion of women have been undergoing BRCA testing in recent years indicates patients (and the physicians who treat them) are following recommendations.
Dr. Shoshana Rosenberg[/caption]
Dr. Shoshana Rosenberg ScD, MPH
Department of Medical Oncology
Dana-Farber Cancer Institute
Boston, Massachusetts
Medical Research: Why would BRCA testing rates have increased among younger women with cancer?
Dr. Rosenberg: There has been increasing awareness surrounding genetic testing for breast cancer in more recent years, likely contributing to the trend that we saw over time in our cohort. This has included more media attention, most notably Angelina Jolie’s sharing her story in 2013.
Medical Research: Is this increase in testing a good thing?
Dr. Rosenberg: Young women who are diagnosed with breast cancer should be getting tested so the fact that an increasing proportion of women have been undergoing BRCA testing in recent years indicates patients (and the physicians who treat them) are following recommendations.
17 Feb Breast Cancer Surgery: Reoperations Less Frequent in High Volume Centers
MedicalResearch.com Interview with: [caption id="attachment_21646" align="alignleft" width="144"] Dr. Art Sedrakyan[/caption]
Dr. Art Sedrakyan MD PhD ScD
Professor of Healthcare Policy and Research in Cardiothoracic Surgery
Department of Public Health
Weill Cornell Medical College
Medical Research: What is the background for this study? What are the main findings?
Dr. Sedrakyan: In the most recent years available to us for research(2011-2013) one in four women underwent repeat surgery within 90 days after breast conserving approach to cancer removal. Patients operated by higher volume physicians had lower chance of undergoing repeat surgery.Uniform guidelines and increased surgical training are needed to standardize the breast conserving surgery to reduce the high rate of repeat surgery.
Dr. Art Sedrakyan[/caption]
Dr. Art Sedrakyan MD PhD ScD
Professor of Healthcare Policy and Research in Cardiothoracic Surgery
Department of Public Health
Weill Cornell Medical College
Medical Research: What is the background for this study? What are the main findings?
Dr. Sedrakyan: In the most recent years available to us for research(2011-2013) one in four women underwent repeat surgery within 90 days after breast conserving approach to cancer removal. Patients operated by higher volume physicians had lower chance of undergoing repeat surgery.Uniform guidelines and increased surgical training are needed to standardize the breast conserving surgery to reduce the high rate of repeat surgery.
13 Feb Breast and Pancreatic Cancer: Pathway Identified That Accelerates Tumors in Obese Patients
Posted at 02:44h
in AACR, Author Interviews, Breast Cancer, Cancer Research, Pancreatic, Weight Research
MedicalResearch.com Interview with:
[caption id="attachment_21566" align="alignleft" width="200"] Dr. Joao Incio[/caption]
Joao Incio, MD
Edwin L. Steele Laboratory for Tumor Biology
Massachusetts General Hospital | Harvard Medical School | Boston, MA, U.S.A
Department of Internal Medicine | Hospital S. Joao | Porto, Portugal
Medical Research: What is the background for this study? What are the main findings?
Dr. Incio: The study focused on the effects of obesity on pancreatic and breast cancer, since more than half of those diagnosed with such tumors are overweight or obese. In addition, a number of large-scale studies have found that obesity leads to an increased risk of death in pancreatic, breast and other types of cancer. But prior to the current study the mechanism of obesity-induced pancreatic and breast cancer progression was unclear. We have uncovered a novel mechanism behind the ability of obesity to promote cancer progression. We found an association between obesity and an overabundance of a factor called PlGF (placental growth factor) and that PlGF’s binding to its receptor VEGFR-1, which is expressed on immune cells within tumors, promotes tumor progression.
We found that obesity increased infiltration of tumor-promoting immune cells and the growth and metastasis of pancreatic cancers. Blocking VEGFR-1 signaling shifted the immune environment towards prevention of tumor progression in obese but not in lean mice in both pancreatic and breast cancer models. We also found that PlGF was present in excess in obesity and that reduction of PlGF produced similar results to VEGFR-1 inhibition in the tumors of obese mice. We also discovered that targeting the PlGF/VEGFR-1 interaction prevents weight gain in a genetically obese mouse model but worsens a diabetes-like condition, a worsening that was alleviated by use of the common diabetes drug metformin, which also had beneficial anti-tumor effects.
Our findings in cellular and animal models, as well as in patient tumor samples, indicate that targeting the PlGF/ VEGFR-1 pathway may be particularly effective in obese patients.
Dr. Joao Incio[/caption]
Joao Incio, MD
Edwin L. Steele Laboratory for Tumor Biology
Massachusetts General Hospital | Harvard Medical School | Boston, MA, U.S.A
Department of Internal Medicine | Hospital S. Joao | Porto, Portugal
Medical Research: What is the background for this study? What are the main findings?
Dr. Incio: The study focused on the effects of obesity on pancreatic and breast cancer, since more than half of those diagnosed with such tumors are overweight or obese. In addition, a number of large-scale studies have found that obesity leads to an increased risk of death in pancreatic, breast and other types of cancer. But prior to the current study the mechanism of obesity-induced pancreatic and breast cancer progression was unclear. We have uncovered a novel mechanism behind the ability of obesity to promote cancer progression. We found an association between obesity and an overabundance of a factor called PlGF (placental growth factor) and that PlGF’s binding to its receptor VEGFR-1, which is expressed on immune cells within tumors, promotes tumor progression.
We found that obesity increased infiltration of tumor-promoting immune cells and the growth and metastasis of pancreatic cancers. Blocking VEGFR-1 signaling shifted the immune environment towards prevention of tumor progression in obese but not in lean mice in both pancreatic and breast cancer models. We also found that PlGF was present in excess in obesity and that reduction of PlGF produced similar results to VEGFR-1 inhibition in the tumors of obese mice. We also discovered that targeting the PlGF/VEGFR-1 interaction prevents weight gain in a genetically obese mouse model but worsens a diabetes-like condition, a worsening that was alleviated by use of the common diabetes drug metformin, which also had beneficial anti-tumor effects.
Our findings in cellular and animal models, as well as in patient tumor samples, indicate that targeting the PlGF/ VEGFR-1 pathway may be particularly effective in obese patients.
11 Feb Meditation May Improve Experience with Imaging-Guided Needle Breast Biopsy
MedicalResearch.com Interview with: [caption id="attachment_21522" align="alignleft" width="133"] Dr. Mary Scott Soo[/caption]
Mary Scott Soo, M.D. FACR
Associate professor of Radiology
Duke Cancer Institute
Medical Research: What is the background for this study?
Dr. Soo: Imaging-guided needle breast biopsies for diagnosing suspicious breast lesions have been performed for many years and have definite advantages as a diagnostic tool over surgical biopsies. These biopsies are performed in outpatient settings, which decrease costs and reduce delays, and are highly accurate and less invasive than surgical procedures, requiring only local anesthesia. However, performing biopsies in this outpatient setting limits the use of intravenous sedation and pain medication that could address commonly experienced patient anxiety and occasional associated pain. Anxiety and pain can negatively impact the patient's experience and could possibly affect the biopsy outcome due to patient movement, and could potentially even alter patients' adherence to follow-up recommendations. Prior studies have explored methods to reduce anxiety, using interventions such as music, hypnosis and anxiolytics. Although hypnosis and anxiolytics are effective, these are a little more complicated to implement due to training costs for administering hypnotherapy, and costs, potential side effects, and need for an adult driver to take the patients home when anxiolytics are used. Other research has shown that meditation-based interventions can lead to positive psychological and physical outcomes, and may be helpful for decreasing anxiety, pain and fatigue.
Loving-kindness mediation is a type of mediation that focuses on relaxation and developing positive emotions, by silently repeating phrases encouraging compassion and goodwill towards oneself and others, while also reducing negative emotions. Previous studies have shown that even a 7-minute loving-kindness meditation can be effective for increasing positive emotions, so my co-authors Rebecca Shelby PhD, a clinical psychologist at Duke’s Pain Prevention and Treatment Research Program,clinical psychologist Anava Wrenn PhD, who has used loving-kindness meditation in a different practice setting, and breast imaging radiologist Jennifer Jarosz MD and I put together a team to study whether an audio-recorded, lovingkindness meditation could reduce anxiety, fatigue and pain during the imaging-guided breast biopsy time frame. We consulted with Mary Brantley, MA, LMFT, who teaches loving-kindness meditation at Duke's Integrative Medicine, to develop an audio-recorded loving-kindness mediation used specifically in the breast biopsy setting, and compared this to using music during biopsies or standard care (supportive dialogue) from the technologist and radiologist performing the biopsy.
Dr. Mary Scott Soo[/caption]
Mary Scott Soo, M.D. FACR
Associate professor of Radiology
Duke Cancer Institute
Medical Research: What is the background for this study?
Dr. Soo: Imaging-guided needle breast biopsies for diagnosing suspicious breast lesions have been performed for many years and have definite advantages as a diagnostic tool over surgical biopsies. These biopsies are performed in outpatient settings, which decrease costs and reduce delays, and are highly accurate and less invasive than surgical procedures, requiring only local anesthesia. However, performing biopsies in this outpatient setting limits the use of intravenous sedation and pain medication that could address commonly experienced patient anxiety and occasional associated pain. Anxiety and pain can negatively impact the patient's experience and could possibly affect the biopsy outcome due to patient movement, and could potentially even alter patients' adherence to follow-up recommendations. Prior studies have explored methods to reduce anxiety, using interventions such as music, hypnosis and anxiolytics. Although hypnosis and anxiolytics are effective, these are a little more complicated to implement due to training costs for administering hypnotherapy, and costs, potential side effects, and need for an adult driver to take the patients home when anxiolytics are used. Other research has shown that meditation-based interventions can lead to positive psychological and physical outcomes, and may be helpful for decreasing anxiety, pain and fatigue.
Loving-kindness mediation is a type of mediation that focuses on relaxation and developing positive emotions, by silently repeating phrases encouraging compassion and goodwill towards oneself and others, while also reducing negative emotions. Previous studies have shown that even a 7-minute loving-kindness meditation can be effective for increasing positive emotions, so my co-authors Rebecca Shelby PhD, a clinical psychologist at Duke’s Pain Prevention and Treatment Research Program,clinical psychologist Anava Wrenn PhD, who has used loving-kindness meditation in a different practice setting, and breast imaging radiologist Jennifer Jarosz MD and I put together a team to study whether an audio-recorded, lovingkindness meditation could reduce anxiety, fatigue and pain during the imaging-guided breast biopsy time frame. We consulted with Mary Brantley, MA, LMFT, who teaches loving-kindness meditation at Duke's Integrative Medicine, to develop an audio-recorded loving-kindness mediation used specifically in the breast biopsy setting, and compared this to using music during biopsies or standard care (supportive dialogue) from the technologist and radiologist performing the biopsy.
29 Jan Radiation Overutilized in Elderly Stage1 ER+ Breast Cancer Patients
MedicalResearch.com Interview with: [caption id="attachment_21108" align="alignleft" width="133"] Dr. Quyen Chu[/caption]
Quyen Chu, MD, MBA, FACS
Charles Knight Professor in Surgery
Professor of Surgery
Chief, Surgical Oncology
Director, Surface Malignancies Program
Feist-Weiller Cancer Center
Louisiana State University
Health Sciences Center, Shreveport
Medical Research: What is the background for this study? What are the main findings?
Dr. Chu: In 2004, national treatment recommendations changed for a select group of elderly breast cancer patients with the Cancer and Leukemia Group B (CALGB) 9343 trial. Research found that postoperative radiation therapy was not needed to prolong survival in a select group of women 70 or older, mainly those with a small, estrogen receptor (ER) positive tumor, and receiving anti-hormone therapy. Even with this information, nearly two thirds of the women who fit these criteria were still receiving radiation therapy after undergoing a lumpectomy although it has been proven to be safe to omit.
We found that as a nation, we are mostly not following the national guideline on breast cancer treatment and that the possible side effects of RT can be avoided.
Medical Research: What should clinicians and patients take away from your report?
Dr. Chu: Clinicians and patients should take away from this report that in U.S. women 70 or older with stage I, ER+ breast cancer and receiving anti-hormone therapy, radiation therapy is overly utilized as it is not needed to prolong survival.
Dr. Quyen Chu[/caption]
Quyen Chu, MD, MBA, FACS
Charles Knight Professor in Surgery
Professor of Surgery
Chief, Surgical Oncology
Director, Surface Malignancies Program
Feist-Weiller Cancer Center
Louisiana State University
Health Sciences Center, Shreveport
Medical Research: What is the background for this study? What are the main findings?
Dr. Chu: In 2004, national treatment recommendations changed for a select group of elderly breast cancer patients with the Cancer and Leukemia Group B (CALGB) 9343 trial. Research found that postoperative radiation therapy was not needed to prolong survival in a select group of women 70 or older, mainly those with a small, estrogen receptor (ER) positive tumor, and receiving anti-hormone therapy. Even with this information, nearly two thirds of the women who fit these criteria were still receiving radiation therapy after undergoing a lumpectomy although it has been proven to be safe to omit.
We found that as a nation, we are mostly not following the national guideline on breast cancer treatment and that the possible side effects of RT can be avoided.
Medical Research: What should clinicians and patients take away from your report?
Dr. Chu: Clinicians and patients should take away from this report that in U.S. women 70 or older with stage I, ER+ breast cancer and receiving anti-hormone therapy, radiation therapy is overly utilized as it is not needed to prolong survival.
23 Jan Nearly 1/3 of Elderly Receive Non-Recommended Cancer Screening Tests
More on Cancer Research on MedicalResearch.com [caption id="attachment_20801" align="alignleft" width="142"] Dr. Firas Abdollah[/caption]
MedicalResearch.com Interview with:
Firas Abdollah, M.D., F.E.B.U.
(Fellow of European Board of Urology) Urology Fellow with the Center for Outcomes Research, Analytics and Evaluation
Vattikuti Urology Institute at Henry Ford Hospital in Detroit
MedicalResearch: What is the background for this study? What are the main findings?
Dr. Abdollah: Cancer screening aims to detect tumors early, before they become symptomatic. Evidence suggests that detection and treatment of early-stage tumors may reduce cancer mortality among screened individuals. Despite this potential benefit, screening programs may also cause harm. Notably, screening may identify low-risk indolent tumors that would never become clinically evident in the absence of screening (overdiagnosis), subjecting patients to the harms of unnecessary treatment. Such considerations are central to screening for prostate and breast cancers, the most prevalent solid tumors in men and women, respectively. These tumors are often slow growing, and guidelines recommend against screening (non-recommended screening) for these tumors in individuals with limited life expectancy, i.e. those with a life expectancy less than 10 years. Unfortunately, our study found that this practice is not uncommon in the US. Using a nationwide representative survey conducted in 2012, we found that among 149,514 individuals 65 years or older, 76,419 (51.1%) received any prostate/breast screening. Among these, 23,532 (30.8%) individuals had a life expectancy of less than 10 years. These numbers imply that among the screened population over 65 years old, almost one in three individuals received a non-recommended screening. This corresponds to an overall rate of non-recommended screening of 15.7% (23,532 of 149,514 individuals).
Another important finding of our study was that there were important variations in the rate of non-recommended screening from state to state; i.e. the chance of an individual older than 65 to receive a non-recommended screening varies based on his/her geographical location in United States.
Finally, on a state-by-state level, there was a correlation (40%) between non-recommended screening for prostate and breast cancer, i.e. states that are more likely to offer non-recommended screening for prostate cancer are also more likely to offer non-recommended screening for breast cancer, and vice versa.
Dr. Firas Abdollah[/caption]
MedicalResearch.com Interview with:
Firas Abdollah, M.D., F.E.B.U.
(Fellow of European Board of Urology) Urology Fellow with the Center for Outcomes Research, Analytics and Evaluation
Vattikuti Urology Institute at Henry Ford Hospital in Detroit
MedicalResearch: What is the background for this study? What are the main findings?
Dr. Abdollah: Cancer screening aims to detect tumors early, before they become symptomatic. Evidence suggests that detection and treatment of early-stage tumors may reduce cancer mortality among screened individuals. Despite this potential benefit, screening programs may also cause harm. Notably, screening may identify low-risk indolent tumors that would never become clinically evident in the absence of screening (overdiagnosis), subjecting patients to the harms of unnecessary treatment. Such considerations are central to screening for prostate and breast cancers, the most prevalent solid tumors in men and women, respectively. These tumors are often slow growing, and guidelines recommend against screening (non-recommended screening) for these tumors in individuals with limited life expectancy, i.e. those with a life expectancy less than 10 years. Unfortunately, our study found that this practice is not uncommon in the US. Using a nationwide representative survey conducted in 2012, we found that among 149,514 individuals 65 years or older, 76,419 (51.1%) received any prostate/breast screening. Among these, 23,532 (30.8%) individuals had a life expectancy of less than 10 years. These numbers imply that among the screened population over 65 years old, almost one in three individuals received a non-recommended screening. This corresponds to an overall rate of non-recommended screening of 15.7% (23,532 of 149,514 individuals).
Another important finding of our study was that there were important variations in the rate of non-recommended screening from state to state; i.e. the chance of an individual older than 65 to receive a non-recommended screening varies based on his/her geographical location in United States.
Finally, on a state-by-state level, there was a correlation (40%) between non-recommended screening for prostate and breast cancer, i.e. states that are more likely to offer non-recommended screening for prostate cancer are also more likely to offer non-recommended screening for breast cancer, and vice versa.
16 Jan Functional Genomics Identifies Genes Essential To Breast Cancer Cell Survival
[caption id="attachment_20692" align="alignleft" width="150"] Dr. Benjamin Neel[/caption]
More on Breast Cancer Research on MedicalResearch.com
MedicalResearch.com Interview with:
Dr. Benjamin Neel MD PhD
Professor, Department of Medicine
Director Perlmutter Cancer Center
NYU Langone Medical Center
Medical Research: What is the background for this study? What are the main findings?
Dr. Neel: Over the past 10 years, there have been major advances in cancer genomics--i.e., defining what changes in genes are found in different types of cancer cells. Sometimes, such studies have resulted in the identification of new drug targets, such as EGF receptor mutations or EML-ALK translocations in lung cancer, RAF mutations in melanoma and hairy cell leukemia, and KIT or PDGFR mutations in GIST. More often, though, either the genetic changes that genomic studies reveal are difficult to target by conventional small molecule drugs or we dont know which of the many mutations found in a given tumor are critical to its proliferation/survival.
"Functional genomics" is a parallel approach to tumor genomics, that aims to use large scale screening technology to identify which genes are essential to cancer cell survival/proliferation. This approach can reveal which genetic changes in cancer cells "drive" the cancer--but it also can find genes on which the cancer becomes dependent because of the other "driver" genes. One major approach to functional genomics uses short hairpin RNAs (a type of RNAinterference/RNAi) to "knock down" the expression of each gene in a cell. Scientists can generate a "library" of designer virus particles, each of which expresses a different hairpin that can "knockdown" a different gene. A large population of tumor cells is then infected with the virus, and scientists use gene sequencing or array based approaches to see which shRNAs become depleted from the starting population of shRNAs; this type of screen is called a "dropout screen".
Earlier studies, including by our group, performed dropout screens on smaller numbers of cancer cell lines. Yet because these screens involved only a few cell lines, they could not represent the large number of sub-types knownt to occur in, for example, breast cancer. Our study, by using 77 breast cancer lines, has adequate power to survey the landscape of breast cancer. Furthermore, by obtaining parallel genomic information, as well as some information on the breast cancer cell "proteome" (the proteins in these cells), we can couple genomic analysis with functional genomics. In addition, we had drug response information for a large number of these lines, and so were able to make some predictions for drugs that might prove additive for breast cancer therapy.
The result is a large number of potential new targets linked to genetic information, as well as new insights into how the different sub-types of breast cancer "rewire" their respective signaling diagrams compared with normal cells.
Dr. Benjamin Neel[/caption]
More on Breast Cancer Research on MedicalResearch.com
MedicalResearch.com Interview with:
Dr. Benjamin Neel MD PhD
Professor, Department of Medicine
Director Perlmutter Cancer Center
NYU Langone Medical Center
Medical Research: What is the background for this study? What are the main findings?
Dr. Neel: Over the past 10 years, there have been major advances in cancer genomics--i.e., defining what changes in genes are found in different types of cancer cells. Sometimes, such studies have resulted in the identification of new drug targets, such as EGF receptor mutations or EML-ALK translocations in lung cancer, RAF mutations in melanoma and hairy cell leukemia, and KIT or PDGFR mutations in GIST. More often, though, either the genetic changes that genomic studies reveal are difficult to target by conventional small molecule drugs or we dont know which of the many mutations found in a given tumor are critical to its proliferation/survival.
"Functional genomics" is a parallel approach to tumor genomics, that aims to use large scale screening technology to identify which genes are essential to cancer cell survival/proliferation. This approach can reveal which genetic changes in cancer cells "drive" the cancer--but it also can find genes on which the cancer becomes dependent because of the other "driver" genes. One major approach to functional genomics uses short hairpin RNAs (a type of RNAinterference/RNAi) to "knock down" the expression of each gene in a cell. Scientists can generate a "library" of designer virus particles, each of which expresses a different hairpin that can "knockdown" a different gene. A large population of tumor cells is then infected with the virus, and scientists use gene sequencing or array based approaches to see which shRNAs become depleted from the starting population of shRNAs; this type of screen is called a "dropout screen".
Earlier studies, including by our group, performed dropout screens on smaller numbers of cancer cell lines. Yet because these screens involved only a few cell lines, they could not represent the large number of sub-types knownt to occur in, for example, breast cancer. Our study, by using 77 breast cancer lines, has adequate power to survey the landscape of breast cancer. Furthermore, by obtaining parallel genomic information, as well as some information on the breast cancer cell "proteome" (the proteins in these cells), we can couple genomic analysis with functional genomics. In addition, we had drug response information for a large number of these lines, and so were able to make some predictions for drugs that might prove additive for breast cancer therapy.
The result is a large number of potential new targets linked to genetic information, as well as new insights into how the different sub-types of breast cancer "rewire" their respective signaling diagrams compared with normal cells.
13 Jan Signaling Pathway Could Be Target of New Triple Negative Breast Cancer Treatment
Click Here for More Articles Related To Breast Cancer on MedicalResearch.com. MedicalResearch.com Interview with: Dr. Chunru Lin PhD Assistant Professor, Department of Molecular and Cellular Oncology, Division of Basic Science Research and Graduate School of Biomedical Sciences The University of Texas MD Anderson Cancer Center, Houston, TX MedicalResearch: What is the background for this study? What are the main findings? Dr. Lin: Triple-Negative Breast Cancer (TNBC) continues to be a serious healthcare problem despite improvements in early detection and treatment; lncRNAs are one of the emerging elements that make the process of understanding breast cancer development and progression so complex yet thorough. Thus, it is imperative to include an examination of lncRNAs when studying breast cancer, especially when researching challenging questions related to relapses and recurrences of breast cancer that occur after targeted therapeutic treatments. A perspective that incorporates lncRNAs into the discussion of breast cancer biology could be the conceptual advance that is necessary to encourage further breakthroughs. Our research reveals the biological functional roles of cytoplasmic lncRNAs as signaling pathway mediators and catalysts that serve as indispensable components of signal transduction cascades and gene networks. This understanding could transform the prevailing dogma of the field of signal transduction. This study has identified a previously unknown mechanism for HIF stabilization and signal transduction, which is triggered by the HB-EGF bound EGFR/GPNMB heterodimer and is mediated by LINK-A-dependent recruitment of two kinases, BRK and LRRK2, to phosphorylate HIF1α at two new sites, leading to HIF1α stabilization and interaction with p300 for transcriptional activation; this further results in cancer glycolytic reprogramming under normoxic conditions. LINK-A is the first demonstrated lncRNA that acts as a key mediator of biological signaling pathways, which suggests the potential for the involvement of other lncRNAs as mediators of numerous signaling pathways. Importantly, expression of LINK-A and activation of the LINK-A mediated signaling pathway are both correlated with TNBC. Targeting LINK-A with LNAs (Locked Nucleic Acids) serves as an encouraging strategy to block reprogramming of glucose metabolism in TNBC with therapeutic potential.12 Jan New Breast Cancer Screening Recommendations Carry Risks Of Later Diagnosis
[caption id="attachment_20523" align="alignleft" width="120"] Dr. Boolbol[/caption]
MedicalResearch.com Interview with:
Susan K. Boolbol, MD, FACS
Chief, Division of Breast Surgery
Chief, Appel-Venet Comprehensive Breast Service
Co-Director, Breast Surgery Fellowship
Mount Sinai Beth Israel
Associate Professor of Surgery
Icahn School of Medicine at Mount Sinai
New York, NY 10003
Medical Research: What is the background for these new recommendations?
Dr. Boolbol: To make this final recommendation, the Task Force conducted a comprehensive review of the science since its 2009 recommendation and considered the public comments it received on its 2015 draft recommendation statement. Based on all of this, the task force issued their recommendations.
Medical Research: What are the main changes from current guidelines?
Dr. Boolbol: Presently, there are several different guidelines and recommendations regarding screening mammography. Depending on the group issuing the guidelines, the recommendations vary from annual mammography beginning at 40 years old to biennial mammograms from 50 to 74 years old. The Task Force continues to find that the benefit of mammography increases with age, and recommends biennial screening in women ages 50 to 74.
Dr. Boolbol[/caption]
MedicalResearch.com Interview with:
Susan K. Boolbol, MD, FACS
Chief, Division of Breast Surgery
Chief, Appel-Venet Comprehensive Breast Service
Co-Director, Breast Surgery Fellowship
Mount Sinai Beth Israel
Associate Professor of Surgery
Icahn School of Medicine at Mount Sinai
New York, NY 10003
Medical Research: What is the background for these new recommendations?
Dr. Boolbol: To make this final recommendation, the Task Force conducted a comprehensive review of the science since its 2009 recommendation and considered the public comments it received on its 2015 draft recommendation statement. Based on all of this, the task force issued their recommendations.
Medical Research: What are the main changes from current guidelines?
Dr. Boolbol: Presently, there are several different guidelines and recommendations regarding screening mammography. Depending on the group issuing the guidelines, the recommendations vary from annual mammography beginning at 40 years old to biennial mammograms from 50 to 74 years old. The Task Force continues to find that the benefit of mammography increases with age, and recommends biennial screening in women ages 50 to 74.
07 Jan Study Finds Regular Mammography May Provide Benefit Up To Age 84
[caption id="attachment_20467" align="alignleft" width="133"] Prof. Hennekens[/caption]
MedicalResearch.com Interview with:
Professor Charles Hennekens MD Dr.P.H
Sir Richard Doll Professor
Senior Academic Advisor to the Dean
Charles E. Schmidt College of Medicine
Florida Atlantic University
777 Glades Road
Boca Raton, FL 33431
Medical Research: What is the background for this study? What are the main findings?
Prof. Hennekens: Randomized evidence indicates clear benefits of mammography in middle age and, at present, most guidelines recommend regular mammography for women up to age 74. In collaboration with colleagues at Baylor Medical College and Meharry Medical School we were able to link the Surveillance, Epidemiology, and End Results (SEER) data to the Medicare administrative claims data. We found that, up to 84 years, screening was more common among whites than blacks and women receiving regular annual screening mammography had lower risks of mortality from breast cancer.
Prof. Hennekens[/caption]
MedicalResearch.com Interview with:
Professor Charles Hennekens MD Dr.P.H
Sir Richard Doll Professor
Senior Academic Advisor to the Dean
Charles E. Schmidt College of Medicine
Florida Atlantic University
777 Glades Road
Boca Raton, FL 33431
Medical Research: What is the background for this study? What are the main findings?
Prof. Hennekens: Randomized evidence indicates clear benefits of mammography in middle age and, at present, most guidelines recommend regular mammography for women up to age 74. In collaboration with colleagues at Baylor Medical College and Meharry Medical School we were able to link the Surveillance, Epidemiology, and End Results (SEER) data to the Medicare administrative claims data. We found that, up to 84 years, screening was more common among whites than blacks and women receiving regular annual screening mammography had lower risks of mortality from breast cancer.
02 Jan Rogue Protein Facilitates Breast Cancer Metastases
[caption id="attachment_20383" align="alignleft" width="300"] Dr. David Gallego Ortega PhD[/caption]
MedicalResearch.com Interview with:
David Gallego Ortega, PhD
Group Leader, Tumour Development Group Cancer Division
Garvan Institute of Medical Research
Conjoint Lecturer, St Vincent’s Clinical School, Faculty of Medicine, UNSW, Australia
National Breast Cancer Foundation and Cure Cancer Foundation Australia Fellow
Medical Research: What is the background for this study? What are the main findings?
Dr. Ortega: We have identified a protein that 'goes rogue’ in breast cancer. The protein, called Elf5, ‘tricks' the immune system producing inflammation so that the immune cells now help the breast cancer cells to spread throughout the body.
Cancer spread, or metastasis, is the ultimate cause of death of breast cancer patients, so we are very excited about our discovery because it opens the door to explore anti-inflammatory drugs that can be combined with existing therapies.
We have found that luminal breast cancer patients that present high levels of Elf5 progress earlier in their disease. The Luminal subtype is the most common type of breast cancer, so these therapies will potentially benefit to 2/3 of all breast cancer patients.
Dr. David Gallego Ortega PhD[/caption]
MedicalResearch.com Interview with:
David Gallego Ortega, PhD
Group Leader, Tumour Development Group Cancer Division
Garvan Institute of Medical Research
Conjoint Lecturer, St Vincent’s Clinical School, Faculty of Medicine, UNSW, Australia
National Breast Cancer Foundation and Cure Cancer Foundation Australia Fellow
Medical Research: What is the background for this study? What are the main findings?
Dr. Ortega: We have identified a protein that 'goes rogue’ in breast cancer. The protein, called Elf5, ‘tricks' the immune system producing inflammation so that the immune cells now help the breast cancer cells to spread throughout the body.
Cancer spread, or metastasis, is the ultimate cause of death of breast cancer patients, so we are very excited about our discovery because it opens the door to explore anti-inflammatory drugs that can be combined with existing therapies.
We have found that luminal breast cancer patients that present high levels of Elf5 progress earlier in their disease. The Luminal subtype is the most common type of breast cancer, so these therapies will potentially benefit to 2/3 of all breast cancer patients.
29 Dec Cancer Stem Cells May Facilitate Recurrent and Metastatic Breast Cancer
[caption id="attachment_20336" align="alignleft" width="200"] Dr. Jenny C. Chang[/caption]
MedicalResearch.com Interview with:
Jenny C. Chang, M.D.
Director, Houston Methodist Cancer Center
Professor of Medicine, Weill Cornell Medical College
Full Member, Houston Methodist Research Institute
Houston, Texas
MedicalResearch: What is the background for this study? What are the main findings?
Dr. Chang: The current treatment of triple negative breast cancer, which accounts for about 15% of all cases of breast cancer, is still based on surgery, radiotherapy, and classic chemotherapy because, unlike other types of breast cancer, it is not amenable to hormonal or targeted therapy. However, research findings suggest that cancer stem cells, which represent about 2% of all neoplastic cells, may play a role in disease relapses and the formation of distant metastases. As these cells may represent a therapeutic target, the aim of this study is to modify the micro-environment in which they reproduce by acting directly on the chemokines involved in inflammation because there is evidence indicating a possible mechanism of action of reparixin, a molecule developed by Dompé, an Italian biopharmaceutical company, in the targeted treatment of these cancers.
Dr. Jenny C. Chang[/caption]
MedicalResearch.com Interview with:
Jenny C. Chang, M.D.
Director, Houston Methodist Cancer Center
Professor of Medicine, Weill Cornell Medical College
Full Member, Houston Methodist Research Institute
Houston, Texas
MedicalResearch: What is the background for this study? What are the main findings?
Dr. Chang: The current treatment of triple negative breast cancer, which accounts for about 15% of all cases of breast cancer, is still based on surgery, radiotherapy, and classic chemotherapy because, unlike other types of breast cancer, it is not amenable to hormonal or targeted therapy. However, research findings suggest that cancer stem cells, which represent about 2% of all neoplastic cells, may play a role in disease relapses and the formation of distant metastases. As these cells may represent a therapeutic target, the aim of this study is to modify the micro-environment in which they reproduce by acting directly on the chemokines involved in inflammation because there is evidence indicating a possible mechanism of action of reparixin, a molecule developed by Dompé, an Italian biopharmaceutical company, in the targeted treatment of these cancers.