MedicalResearch.com Interview with:
[caption id="attachment_35660" align="alignleft" width="132"]

Dr. Ratanawongsa[/caption]
Neda Ratanawongsa, MD, MPH
Associate Chief Health Informatics Officer for Ambulatory Services, San Francisco Health Network
Associate Professor, Division of General Internal Medicine
UCSF Center for Vulnerable Populations
Physician, Richard H. Fine People's Clinic (RHPC)
Zuckerberg San Francisco General Hospital
San Francisco, CA 94110
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: U.S. federal incentives allowed many safety net healthcare systems to afford fully functional electronic health record systems (EHRs). Although EHRs can help clinicians provide care to vulnerable populations, clinicians may struggle with managing the EHR workload, particularly in resource-limited settings. In addition, clinicians’ use of EHRs during clinic visits may affect how they communicate with patients.
There are two forms of EHR use during clinic visits. Clinicians can
multitask, for example, by ordering laboratory tests while chatting with a patient about baseball. However, like distracted driving, using EHRs while talking with increases risks – in this case, the risk of errors in patient-provider communication or in the EHR task. Alternatively, clinicians can
use EHRs in complete silence, which may be appropriate for high-risk tasks like prescribing insulin. However, silence during visits has been associated with lower patient satisfaction and less patient-centered communication.
So we studied how primary and specialty care clinicians used EHRs during visits with English- and Spanish-speaking patients in a safety net system with an EHR certified for Centers for Medicare & Medicaid Services meaningful use incentive programs. We found that multitasking EHR use was more common than silent EHR use (median of 30.5% vs. 4.6% of visit time). Focused patient-clinician talk comprised one-third of visit time.
We also examined the transitions into and out of silent EHR use. Sometimes clinicians explicitly stated a need to focus on the
EHR, but at times, clinicians drifted into silence without warning. Patients played a role in breaking silent EHR use, either by introducing small talk or by bringing up their health concerns.


 Dr. McPeek Hinz[/caption]
Eugenia McPeek Hinz MD MS FAMIA
Associate CMIO - DHTS
Duke University Health System
MedicalResearch.com: What is the background for this study?
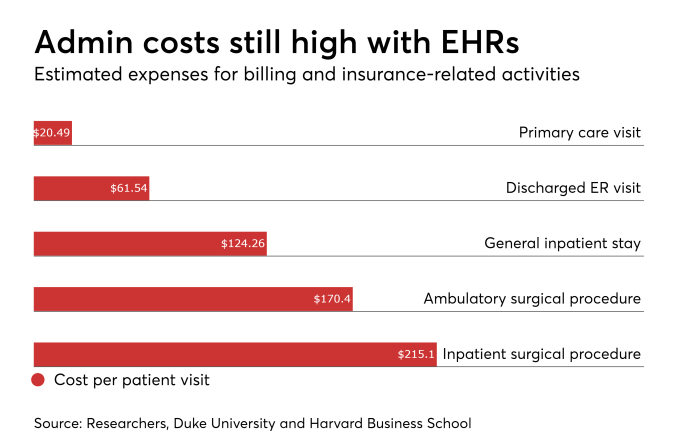
Response: Clinician burnout rates have hovered around 50% for much of the past decade. Burnout is a significant concern in healthcare for its effects on care givers and associated downstream adverse implications on patient care for quality and safety. The ubiquitous presence of Electronic Health Records (EHR) along with the increased clerical components and after hours use has been a significant concern for contributing to provider burnout.
Dr. McPeek Hinz[/caption]
Eugenia McPeek Hinz MD MS FAMIA
Associate CMIO - DHTS
Duke University Health System
MedicalResearch.com: What is the background for this study?
Response: Clinician burnout rates have hovered around 50% for much of the past decade. Burnout is a significant concern in healthcare for its effects on care givers and associated downstream adverse implications on patient care for quality and safety. The ubiquitous presence of Electronic Health Records (EHR) along with the increased clerical components and after hours use has been a significant concern for contributing to provider burnout.









 Dr. Gardner[/caption]
Rebekah L Gardner MD
Associate Professor of Medicine
Warren Alpert Medical School
Brown University
Providence, Rhode Island
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Burnout profoundly affects physicians, their patients, and the health care system.The role of technology in physician burnout, specifically health information technology (HIT), is not as well characterized as some of the other factors. We sought to understand how stress related to HIT use predicts burnout among physicians.
Our main findings are that 70% of electronic health record (EHR) users reported HIT-related stress, with the highest prevalence in primary care-oriented specialties. We found that experiencing HIT-related stress independently predicted burnout in these physicians, even accounting for other characteristics like age, gender, and practice type. In particular, those with time pressures for documentation or those doing excessive “work after work” on their EHR at home had approximately twice the odds of burnout compared to physicians without these challenges. We found that physicians in different specialties had different rates of stress and burnout.
Dr. Gardner[/caption]
Rebekah L Gardner MD
Associate Professor of Medicine
Warren Alpert Medical School
Brown University
Providence, Rhode Island
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Burnout profoundly affects physicians, their patients, and the health care system.The role of technology in physician burnout, specifically health information technology (HIT), is not as well characterized as some of the other factors. We sought to understand how stress related to HIT use predicts burnout among physicians.
Our main findings are that 70% of electronic health record (EHR) users reported HIT-related stress, with the highest prevalence in primary care-oriented specialties. We found that experiencing HIT-related stress independently predicted burnout in these physicians, even accounting for other characteristics like age, gender, and practice type. In particular, those with time pressures for documentation or those doing excessive “work after work” on their EHR at home had approximately twice the odds of burnout compared to physicians without these challenges. We found that physicians in different specialties had different rates of stress and burnout.







 Dr. David Ouyang[/caption]
MedicalResearch.com Interview with:
David Ouyang MD
Department of Internal Medicine
Stanford University School of Medicine
Stanford, California
Medical Research: What is the background for this study? What are the main findings?
Dr. Ouyang: In American teaching hospitals, trainee resident physicians are an integral part of the medical team in performing procedures, writing notes, and coordinating care. As more care is being facilitated by electronic medical record (EMR) systems, we are just now finally able to understand how much residents work and how residents spend their time. In our study, we examined the types and timing of electronic actions performed on the EMR system by residents and found that residents spend about a third (36%) of their day in front of the computer and frequently perform many simultaneous tasks across the charts of multiple patients. Additionally, residents often do work long hours, with a median of 69.2 hours per week when on the inpatient medicine service.
Dr. David Ouyang[/caption]
MedicalResearch.com Interview with:
David Ouyang MD
Department of Internal Medicine
Stanford University School of Medicine
Stanford, California
Medical Research: What is the background for this study? What are the main findings?
Dr. Ouyang: In American teaching hospitals, trainee resident physicians are an integral part of the medical team in performing procedures, writing notes, and coordinating care. As more care is being facilitated by electronic medical record (EMR) systems, we are just now finally able to understand how much residents work and how residents spend their time. In our study, we examined the types and timing of electronic actions performed on the EMR system by residents and found that residents spend about a third (36%) of their day in front of the computer and frequently perform many simultaneous tasks across the charts of multiple patients. Additionally, residents often do work long hours, with a median of 69.2 hours per week when on the inpatient medicine service.


