For many years now, professional nursing has held a unique place in the American health care system. Nurses make up one of the largest health care professions in the U.S. with more than 3.1 million nurses working in diverse fields and settings.
Although most nurses work in health care settings like hospitals, a nurse’s expertise expands well beyond the hospital walls. Working on their own and alongside other healthcare professionals, nurses promote the health of families, individuals, and communities.
Nurses have always played an important role in healthcare settings. However, their role has changed a lot over the years. In the past, nurses had extraordinarily little formal medical training. In fact, nurses learned the medical skills they needed from their mothers or other women in the nursing profession.
Today, the nursing profession has changed for the better. Not only are there extensive training programs available for nurses, but this role now comes with a level of prestige that was not there before. And this is not the only thing that has altered. Technology has also played a huge role in changing this profession for the better. Keep reading below to find out about the history of nursing and how technology has changed the role of nursing. For those seeking additional assistance or support in navigating the complexities of nursing education or academic tasks, exploring resources from reputable
nursing paper writing services can offer valuable expertise and assistance in achieving success in the field.
How Nursing Has Changed Over Time
Time has done a lot for many career paths. However, the nursing profession has seen more changes than most. Here are some of the ways the nursing profession has changed over time:
Training – in the past, nurses were not required to have any formal education. However, nowadays nurses are no longer able to care for patients without passing the correct certification first.
Setting – many years ago, nurses would take care of people in their homes or on the battlefield. Although some nurses still care for patients in their homes, nowadays, most nurses work in a hospital setting.
Responsibilities – nursing responsibilities have come a long way from the early days when they used to look a lot like a household chore list. The change in responsibilities for nurses stems from several changes in the profession, including the changing views of women, more comprehensive training, and the growing demand for medical professionals.
Culture – in the 20
th century, nursing culture was known as being mainly made up of females who had a small amount of medical knowledge. While nursing culture has not changed completely, it has changed a lot over the years. In fact, research suggests that more men than ever are choosing to train in this profession.
Patient care – patient care is more important than ever before. The advancements in technology have created an environment that makes patient care more helpful and efficient for patients. These advancements have altered almost every industry in the U.S. and the medical field is no different.




 Dr. Khullar[/caption]
Dhruv Khullar, M.D., M.P.P.
Director of Policy Dissemination
Physicians Foundation Center for Physician Practice and Leadership
Assistant Professor of Health Policy and Economics
Weill Cornell Medicine, NYC
MedicalResearch.com: What is the background for this study?
Response: From prior research, we know that there are racial/ethnic differences in the acute impact of COVID-19, including higher rates of hospitalization and death among Black and Hispanic individuals compared to white individuals. Less is known about whether there are differences in the rates or types of long COVID by race and ethnicity.
Dr. Khullar[/caption]
Dhruv Khullar, M.D., M.P.P.
Director of Policy Dissemination
Physicians Foundation Center for Physician Practice and Leadership
Assistant Professor of Health Policy and Economics
Weill Cornell Medicine, NYC
MedicalResearch.com: What is the background for this study?
Response: From prior research, we know that there are racial/ethnic differences in the acute impact of COVID-19, including higher rates of hospitalization and death among Black and Hispanic individuals compared to white individuals. Less is known about whether there are differences in the rates or types of long COVID by race and ethnicity.



 Dr. McPeek Hinz[/caption]
Eugenia McPeek Hinz MD MS FAMIA
Associate CMIO - DHTS
Duke University Health System
MedicalResearch.com: What is the background for this study?
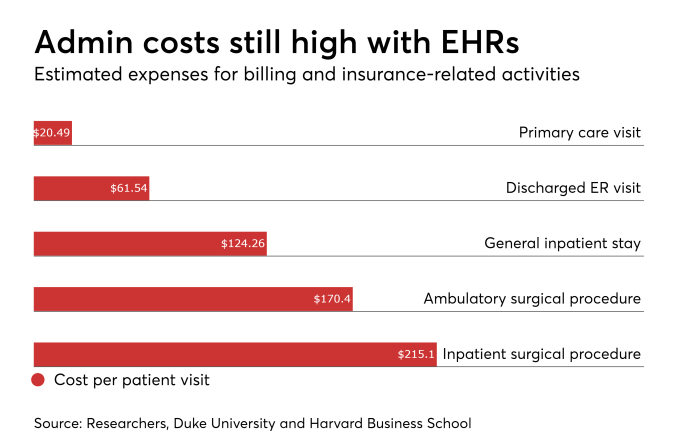
Response: Clinician burnout rates have hovered around 50% for much of the past decade. Burnout is a significant concern in healthcare for its effects on care givers and associated downstream adverse implications on patient care for quality and safety. The ubiquitous presence of Electronic Health Records (EHR) along with the increased clerical components and after hours use has been a significant concern for contributing to provider burnout.
Dr. McPeek Hinz[/caption]
Eugenia McPeek Hinz MD MS FAMIA
Associate CMIO - DHTS
Duke University Health System
MedicalResearch.com: What is the background for this study?
Response: Clinician burnout rates have hovered around 50% for much of the past decade. Burnout is a significant concern in healthcare for its effects on care givers and associated downstream adverse implications on patient care for quality and safety. The ubiquitous presence of Electronic Health Records (EHR) along with the increased clerical components and after hours use has been a significant concern for contributing to provider burnout. 
 Dr. Traverso[/caption]
Carlo Giovanni Traverso, MB, BChir, PhD
Associate Physician, Brigham and Women's Hospital
Assistant Professor,
[caption id="attachment_56823" align="alignleft" width="150"]
Dr. Traverso[/caption]
Carlo Giovanni Traverso, MB, BChir, PhD
Associate Physician, Brigham and Women's Hospital
Assistant Professor,
[caption id="attachment_56823" align="alignleft" width="150"] Dr. Chai[/caption]
Peter R. Chai, MD, MMS
Emergency Medicine Physician and Medical Toxicologist
Harvard Medical School
Brigham and Women's Hospital
Department of Medicine
Dr. Chai[/caption]
Peter R. Chai, MD, MMS
Emergency Medicine Physician and Medical Toxicologist
Harvard Medical School
Brigham and Women's Hospital
Department of Medicine
 MedicalResearch.com: What is the background for this study? What are some of the functions that Dr. Spot can facilitate?
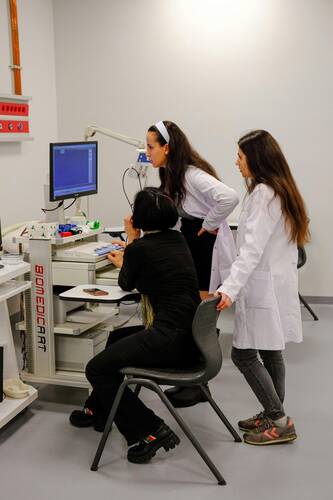
Response: During the COVID-19 pandemic, we wanted to consider innovative methods to provide additional social distance for physicians evaluating low acuity individuals who may have COVID-19 disease in the emergency department. While other health systems had instituted processes like evaluating patients from outside of emergency department rooms or calling patients to obtain a history, we considered the use of a mobile robotic system in collaboration with Boston Dynamics to provide telemedicine triage on an agile platform that could be navigated around a busy emergency department. Dr. Spot was built with a camera system to help an operator navigate it through an emergency department into a patient room where an on-board tablet would permit face-to-face triage and assessment of individuals.
MedicalResearch.com: What is the background for this study? What are some of the functions that Dr. Spot can facilitate?
Response: During the COVID-19 pandemic, we wanted to consider innovative methods to provide additional social distance for physicians evaluating low acuity individuals who may have COVID-19 disease in the emergency department. While other health systems had instituted processes like evaluating patients from outside of emergency department rooms or calling patients to obtain a history, we considered the use of a mobile robotic system in collaboration with Boston Dynamics to provide telemedicine triage on an agile platform that could be navigated around a busy emergency department. Dr. Spot was built with a camera system to help an operator navigate it through an emergency department into a patient room where an on-board tablet would permit face-to-face triage and assessment of individuals.














 Dr. Gardner[/caption]
Rebekah L Gardner MD
Associate Professor of Medicine
Warren Alpert Medical School
Brown University
Providence, Rhode Island
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Burnout profoundly affects physicians, their patients, and the health care system.The role of technology in physician burnout, specifically health information technology (HIT), is not as well characterized as some of the other factors. We sought to understand how stress related to HIT use predicts burnout among physicians.
Our main findings are that 70% of electronic health record (EHR) users reported HIT-related stress, with the highest prevalence in primary care-oriented specialties. We found that experiencing HIT-related stress independently predicted burnout in these physicians, even accounting for other characteristics like age, gender, and practice type. In particular, those with time pressures for documentation or those doing excessive “work after work” on their EHR at home had approximately twice the odds of burnout compared to physicians without these challenges. We found that physicians in different specialties had different rates of stress and burnout.
Dr. Gardner[/caption]
Rebekah L Gardner MD
Associate Professor of Medicine
Warren Alpert Medical School
Brown University
Providence, Rhode Island
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Burnout profoundly affects physicians, their patients, and the health care system.The role of technology in physician burnout, specifically health information technology (HIT), is not as well characterized as some of the other factors. We sought to understand how stress related to HIT use predicts burnout among physicians.
Our main findings are that 70% of electronic health record (EHR) users reported HIT-related stress, with the highest prevalence in primary care-oriented specialties. We found that experiencing HIT-related stress independently predicted burnout in these physicians, even accounting for other characteristics like age, gender, and practice type. In particular, those with time pressures for documentation or those doing excessive “work after work” on their EHR at home had approximately twice the odds of burnout compared to physicians without these challenges. We found that physicians in different specialties had different rates of stress and burnout.