MedicalResearch.com Interview with:
[caption id="attachment_49973" align="alignleft" width="163"]

Dr. Nemesure[/caption]
Barbara Nemesure, PhD
Professor, Department of Family, Population and Preventive Medicine
Division Head, Epidemiology and Biostatistics
Director, Cancer Prevention and Control Program
Director, Lung Cancer Program, Stony Brook Cancer Center
Renaissance School of Medicine
Stony Brook University
MedicalResearch.com: What is the background for this study? What are the main findings?
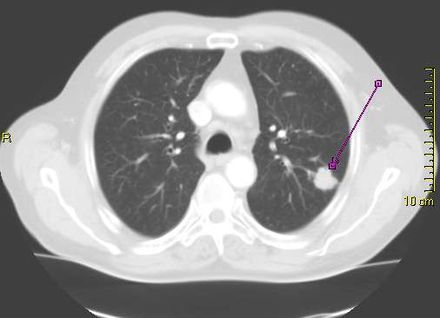
Response: Lung cancer is the most common cause of cancer death, claiming the lives of more than 150,000 people in the United States each year. While lung nodules are not uncommon, it has remained a challenge to differentiate those that will progress to cancer and those that will remain benign. Although numerous risk prediction models for lung cancer have been developed over the past 2 decades, the majority have been based on retrospective analyses or high risk groups with a strong history of tobacco use. To date, there have been a limited number of large-scale, prospective studies evaluating risk that a nodule will convert to cancer in the general population.
This investigation aimed to construct a population-based risk prediction model of incident lung cancer for patients found to have a lung nodule on initial CT scan. The derived model was determined to have high accuracy for predicting nodule progression to cancer and identified a combination of clinical and radiologic predictors including age, smoking history (pack-years), a personal history of cancer, the presence of chronic obstructive pulmonary disease (COPD), and nodule features such as size, presence of spiculation and ground glass opacity type.
When compared to patients in the low risk category, those defined as high risk had more than 14 times the risk of developing lung cancer. Quantification of reliable risk scores has high clinical utility, enabling physicians to better stratify treatment plans for their patients.



 Dr. Campanella[/caption]
Gabriele Campanella, PhD
Assistant Professor
Windreich Department of Artificial Intelligence and Human Health
Icahn School of Medicine at Mount Sinai
MedicalResearch.com: What is the background for this study?
Response: Lung cancer is the most lethal cancer in the US. Lung adenocarcinoma (LUAD) is the most common form of lung cancer with an incidence of over 100k per year in the US. EGFR mutations are common driver mutations in LUAD, and importantly, these mutations can be targeted by TKI therapy, which has high response rates. Because of this, EGFR testing via NGS (Next Generation Sequencing) is considered mandatory by guidelines for any LUAD diagnosis.
In high-resource settings, rapid EGFR testing is done while waiting for confirmation via NGS. This is because NGS takes about 2 weeks on average, while the rapid testing has a median TAT of 2 days. Early treatment decisions could be made based on the rapid test results. Rapid tests have some important drawbacks, most notably, it exhausts tissue. In lung cancer, tissue is scarce in the first place, and up to 25% of cases, after rapid testing there is not enough tissue for NGS. In those circumstances, patients have to be biopsied again, which adds unnecessary risk for the patient. Even worse, in some cases, the NGS is never done. A non-tissue-exhaustive computational biomarker could be used instead of the tissue-based rapid test.
Dr. Campanella[/caption]
Gabriele Campanella, PhD
Assistant Professor
Windreich Department of Artificial Intelligence and Human Health
Icahn School of Medicine at Mount Sinai
MedicalResearch.com: What is the background for this study?
Response: Lung cancer is the most lethal cancer in the US. Lung adenocarcinoma (LUAD) is the most common form of lung cancer with an incidence of over 100k per year in the US. EGFR mutations are common driver mutations in LUAD, and importantly, these mutations can be targeted by TKI therapy, which has high response rates. Because of this, EGFR testing via NGS (Next Generation Sequencing) is considered mandatory by guidelines for any LUAD diagnosis.
In high-resource settings, rapid EGFR testing is done while waiting for confirmation via NGS. This is because NGS takes about 2 weeks on average, while the rapid testing has a median TAT of 2 days. Early treatment decisions could be made based on the rapid test results. Rapid tests have some important drawbacks, most notably, it exhausts tissue. In lung cancer, tissue is scarce in the first place, and up to 25% of cases, after rapid testing there is not enough tissue for NGS. In those circumstances, patients have to be biopsied again, which adds unnecessary risk for the patient. Even worse, in some cases, the NGS is never done. A non-tissue-exhaustive computational biomarker could be used instead of the tissue-based rapid test.

 Dr. Han[/caption]
Summer S Han, PhD
Associate Professor
Dr. Han[/caption]
Summer S Han, PhD
Associate Professor
 Dr. Choi[/caption]
Dr. Eunji Choi PhD
Instructor, Neurosurgery
Department: Adult Neurosurgery
Stanford University School of Medicine
MedicalResearch.com: What is the background for this study?
Dr. Choi[/caption]
Dr. Eunji Choi PhD
Instructor, Neurosurgery
Department: Adult Neurosurgery
Stanford University School of Medicine
MedicalResearch.com: What is the background for this study?
 Dr. Lova Sun[/caption]
Lova L. Sun, MD, MSCE
Medical Oncology
Assistant Professor of Medicine
Hospital of the University of Pennsylvania
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: An common clinical question for patients with metastatic non-small cell lung cancer with long-term response to immunotherapy-based treatment is how long to continue treatment. The major clinical trials stopped immunotherapy at a maximum of 2 years, but in clinical practice many patients and clinicians continue treatment beyond this time point.
We conducted a retrospective study of lung cancer patients across the US with long-term response to immunotherapy, to compare survival between those who stopped treatment at 2 years vs those who continued beyond 2 years. We found that there was no statistically significant difference in survival between the two groups.
Dr. Lova Sun[/caption]
Lova L. Sun, MD, MSCE
Medical Oncology
Assistant Professor of Medicine
Hospital of the University of Pennsylvania
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: An common clinical question for patients with metastatic non-small cell lung cancer with long-term response to immunotherapy-based treatment is how long to continue treatment. The major clinical trials stopped immunotherapy at a maximum of 2 years, but in clinical practice many patients and clinicians continue treatment beyond this time point.
We conducted a retrospective study of lung cancer patients across the US with long-term response to immunotherapy, to compare survival between those who stopped treatment at 2 years vs those who continued beyond 2 years. We found that there was no statistically significant difference in survival between the two groups.
 Dr. Sally Lau[/caption]
Dr. Sally Lau MD
Medical oncologist, NYU Langone’s Perlmutter Cancer Center
Assistant professor of medicine
NYU Grossman School of Medicine
MedicalResearch.com: How big is the problem of
Dr. Sally Lau[/caption]
Dr. Sally Lau MD
Medical oncologist, NYU Langone’s Perlmutter Cancer Center
Assistant professor of medicine
NYU Grossman School of Medicine
MedicalResearch.com: How big is the problem of 

 Dr. Barry[/caption]
Michael J. Barry, M.D
Director of the Informed Medical Decisions Program
Health Decision Sciences Center
Massachusetts General Hospital.
Professor of medicine at Harvard Medical School
Dr. Barry was appointed as Vice Chair of USPSTF in March 2021.
He previously served as a member from January 2017 through December 2020.
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: The Task Force looked at the use of vitamin and mineral supplementation specifically for the prevention of heart disease, stroke, and cancer. We found that there is not enough evidence to recommend for or against taking multivitamin supplements, nor the use of single or paired nutrient supplements, to prevent these conditions.
However, we do know that you should not take vitamin E or beta-carotene for this purpose.
Dr. Barry[/caption]
Michael J. Barry, M.D
Director of the Informed Medical Decisions Program
Health Decision Sciences Center
Massachusetts General Hospital.
Professor of medicine at Harvard Medical School
Dr. Barry was appointed as Vice Chair of USPSTF in March 2021.
He previously served as a member from January 2017 through December 2020.
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: The Task Force looked at the use of vitamin and mineral supplementation specifically for the prevention of heart disease, stroke, and cancer. We found that there is not enough evidence to recommend for or against taking multivitamin supplements, nor the use of single or paired nutrient supplements, to prevent these conditions.
However, we do know that you should not take vitamin E or beta-carotene for this purpose.