MedicalResearch.com Interview with:
Neda Ratanawongsa, MD, MPH
CMIO for CareLinkSF
Associate Professor, Division of General Internal Medicine
UCSF Center for Vulnerable Populations
Physician, Richard H. Fine People's Clinic (RHPC)
San Francisco, CA 94110
Medical Research: What is the background for this study?
Dr. Ratanawongsa: Many people are concerned about the growing intrusion of computers into the patient-provider relationship. Touted as systems that will make care safer and more cost-effective, electronic health records (EHRs) have proliferated rapidly across the country, fueled by HITECH funding. However, some health care professionals feel like computers keep them from connecting with their patients. Also prior research has shown that computer use can change communication in the exam room and shift agenda from patients' concerns toward medical talk.
Safety net patients already face communication barriers in routine care, particularly language and literacy barriers. Although EHRs could help improve care and communication with these vulnerable patients by helping clinicians fill in the gaps (e.g., what happened in the ED, what medication were you given by that specialist), EHRs could also worsen communication by drawing clinicians' focus away from patients during visits.
(more…)
MedicalResearch.com Interview with:
Jonathan R. Enriquez, MD
Assistant Professor of Medicine
Division of Cardiology
University of Missouri- Kansas City
Director, Coronary Care Unit
Truman Medical CenterMedical Research: What is the background for this study? Dr. Enriquez:
In 2009, U.S. legislation appropriated tens of billions of dollars to promote the use of electronic health records (EHRs).
Approximately 4 million hospitalizations for cardiovascular diagnoses occur annually in the U.S., which are more hospitalizations than for any other category of disease. Therefore, evaluating the use of EHRs in these settings can help us understand how to best optimize the care and outcomes of a huge set of patients.
MedicalResearch.com Interview with:
Dr. Pablo Moreno Franco MD
Assistant Professor of Medicine
MAYO Clinic
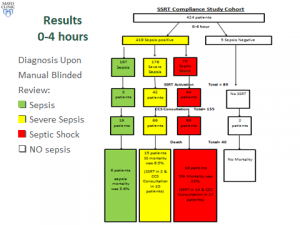
Medical Research: What is the background for this study? What are the main findings?
Dr. Pablo Franco: Early alerts and prompt management of patient with severe sepsis and septic shock (SS/S) starting in the emergency department (ED) have been shown to improve mortality and other pertinent outcomes. With this in mind, we formed a multidisciplinary sepsis and shock response team (SSRT) in September 2013. Automated electronic sniffer alerted ED providers for possible sepsis and when S/SS was identified, they were encouraged to activate SSRT.
Two blinded reviewers retrospectively abstracted data on clinical trajectory and outcomes of all patients with sepsis and SS/S admitted at a single academic medical center between September 2013 and September 2014. Given importance of timely recognition and interventions in S/SS, we specifically focused on 2 periods: 0-4 hours and 4-12 hours after hospital admission. Additionally, we compared the compliance to “standard of care” between the SSRT pre-implementation period and the study period.
There were 167 patients admitted with sepsis, among which there were 3 SSRT activations and sepsis mortality was 3.6%. There were 176 patients with SS, SSRT was called in 42 (23%) and SS mortality was 8.5%. CCS was involved in 66 patients and mortality was 6.9% if SSRT was activated, versus 21.6% if SSRT was not activated. There were 76 patients with septic shock, SSRT was called in 44 (57%) and septic shock mortality was 25%. Critical Care Service (CCS) was involved in 68 patients and mortality rates with and without SSRT were 30.9% and 15.4%, respectively. The all-or-none compliance with applicable goals of resuscitation improved from the baseline 0% to over 50% at the study period end. Overall observed/expected sepsis mortality index improved from 1.38 pre-SSRT to 0.68 post-SSRT implementation.
(more…)
MedicalResearch.com Interview with:
Talley Holman, PhD, MBA
Senior eHealth Systems Analyst, Practice Advancement
American Academy of Family Physicians
Leawood, KS 66211 and
John Beasley MD
Professor of Family Medicine
School of Medicine and Public Health and the
Department of Industrial and Systems Engineering
University of Wisconsin Madison, WI
Medical Research: What is the background for this study?
Dr. Holman: From an engineering standpoint, tools such as EHRs are designed based on objectives, and the workflows that are created are developed to achieve those objectives. In health care, workflows have not been well understood, so designers have made assumptions when pressed to create tools to address specific situations, problems, or issues. However, the effectiveness of many of these tools is lacking, based on feedback. This led us to take a step back and ask if there is a standard workflow, and if so, what is it?
Dr. Beasley: Physicians (and staff) have noted that the EHR is not doing a good job of supporting their work - and changes are made that appear to disrupt the physician’s workflow. There appears to have been an assumption on the part of designers/implementers that workflow is linear.
(more…)
MedicalResearch.com Interview with:
Lara Varpio, PhDAssociate Professor, Department of MedicineActing Associate Director, Graduate Programs in Health Professions EducationUniformed Services University of the Health Sciences
Bethesda MD and
Dr. Judy Rashotte PhD
Director Nursing Research and Knowledge Translation Consultant Ottawa Canada
Medical Research: What is the background for this study? Drs. Varpio and Rashotte: Electronic health records (EHRs) are being adopted in healthcare centers around the world. The patient record is intricately implicated in care processes, clinical reasoning activities, and in collaborative work. As part of a larger study aimed at understanding how EHRs impact health professionals’ interprofessional collaborative practice (ICP), we explored how changing from a paper chart to an EHR can impact clinical reasoning.
Medical Research: What are the main findings?Drs. Varpio and Rashotte: Our research demonstrated how different parts of the patient record (i.e. communication genres / artefacts) are part of the contextual factors that influence clinical reasoning and ICP. A key finding of our study is that building the patient’s story is an essential part of clinical reasoning activities. Making and understanding data interconnections is facilitated when clinicians are actively engaged in assembling isolated data bits into contextually-derived, comprehensive, and comprehensible ensembles. Building the patient’s story is facilitated through the use of a chronologically-organized textual narrative (i.e. free-text notations) structure and structures that promote visual bundles of clinical data. The use of an EHR can problematize clinicians’ ability to build the patient’s story and to disseminate it with other members of the care team when data interconnections are fragmented. Fragmentation happens when narrative spaces are dispersed and/or character-limited, and when data displays are not chronologically organized in visual assemblies. The constraint of chronologically and contextually isolated data inhibits clinicians’ ability to read the why and how interpretations of clinical activities from other team members. When an EHR splinters narrative reports, there is a loss of shared interprofessional understanding of the patient’s story, and time efficient care delivery can be compromised.
(more…)
MedicalResearch.com Interview with:
Professor Susan A. Sherer, Ph.D.
Lehigh University
College of Business and Economics
Department of Management
Bethlehem, PA 18015MedicalResearch: What is the background for this study? What are the main findings?Dr. Sherer: With the growth in electronic health record implementation, there has been increasing demand for integration of these records within and across practice settings that have different work cultures, e.g. ambulatory and hospital locations. We find that computer integration alone does not result in coordination; users must value the integrated information and incorporate this information within their workflows. Users must move beyond technology acceptance and adaptation to focus on and value coordination. The system itself cannot drive these process changes; specific work process changes must be instituted and the users must adapt these changes.
(more…)
MedicalResearch.com Interview with:
Hardeep Singh, MD MPH
Chief, Health Policy, Quality and Informatics Program,
Houston Veterans Affairs Health Services Research Center for Innovations
Michael E. DeBakey Veterans Affairs Medical Center and
Baylor College of Medicine
Houston TX 77030
Medical Research: What is the background for this study? What are the main findings?
Dr. Singh: Missed or delayed diagnoses are among the most common patient safety concerns in outpatient settings, and measuring and reducing them is a high priority. Our computerized triggers scanned huge amounts of patient data in the electronic health record and flagged individuals at risk for delays in follow-up of cancer-related abnormal clinical findings. Records of all patients flagged by the computerized trigger algorithm in the intervention group were reviewed to determine the presence of delay and if delay was confirmed, we communicated this information to their clinicians. We found that patients seeing clinicians who were notified of potential delays had more timely diagnostic evaluation for both prostate and colon cancer and more patients in the intervention part of the study had received diagnostic evaluation by the time we completed our final review.
(more…)
MedicalResearch.com Interview with:
Nisha C. Hazra MSc
Department of Primary Care and Public Health Sciences,
King's College London, London, UK
Medical Research: What is the background for this study? What are the main findings?
Response: Our study was motivated by limited evidence about the health status of very old people, the fastest growing group of the UK population with significant implications for future NHS health-care costs. Our findings indicated an increasing number of people reaching the age of 100 years, with the increase being higher among women comparing to men (a ratio of 4 to 1). Another interesting finding was that men reaching 100 years tended to be healthier than their female counterparts. In particular, women were more likely to present multiple chronic diseases compared to men and tended to be more frail, experiencing more falls, fractures, incontinence and hearing/visual impairments.
(more…)
MedicalResearch.com Interview with:
Dr. Courtney Lyles Ph.D.
Assistant Professor
UCSF School of Medicine
Medical Research: What is the background for this study? What are the main findings?
Dr. Lyles: In our commentary (http://www.plosmedicine.org/article/info%3Adoi%2F10.1371%2Fjournal.pmed.1001852), we describe the Meaningful Use program sponsored by the federal government to incentivize healthcare systems to implement electronic health records (EHRs). This Meaningful Use program also includes financial incentives for healthcare systems who can get substantial proportions of their patient population to access their electronic health records – that is, by logging into an online patient portal website to view medical information like lab results or immunization lists or to perform a healthcare task like requesting a medication refill or messaging their provider. Because there are billions of dollars at stake in this program for EHR implementation, there is a lot of attention on this issue right now. Many thought leaders are discussing how we can transform healthcare by digitizing medical information and connecting with patients in their everyday life outside of office or hospital visits. Portals are key to a lot of changes we might make in healthcare delivery in an attempt to increase convenience and satisfaction for patients. Perhaps most importantly, these online portal websites are also one of the first health technologies that will be relatively uniformly distributed across healthcare settings, from private doctor’s offices to public clinics/hospitals serving vulnerable patient populations.
However, our main message is that we in the medical and healthcare fields should be paying more attention to how patients are able to understand and use the information provided through portal websites. There is a lot of evidence that patients who have lower education/income, are from racial/ethnic minority groups, or have limited health literacy are significantly less likely to use the existing portal websites. There is also evidence that portal websites are not extremely usable or accessible, which is an additional barrier for those with communication barriers like lower literacy or limited English proficiency. Therefore, we don’t want widespread EHR implementation to result in only the most well-resourced individuals gaining the potential benefits of portal access.
(more…)
MedicalResearch.com Interview with:
Dawn Heisey-Grove, MPH
Office of Planning, Evaluation, and Analysis Office of the National Coordinator for Health Information Technology U.S....
MedicalResearch.com Interview with:
Elliot B Tapper, M.D.
Clinical Fellow in Medicine (EXT)
Beth Israel Deaconess Medical Center
Boston MA 02215
Medical Research: What is...
MedicalResearch.com Interview with:
Karen E. Joynt, MD MPH
Cardiovascular Division,
Brigham and Women's Hospital and VA Boston Healthcare System
Department of Health Policy and Management
Harvard T.H. Chan School of Public Health
MedicalResearch: What is the background for this study? What are the main findings?Dr. Joynt: While there is a great deal of optimism about the potential of Electronic Health Records (EHRs) to improve health care, there is little national data examining whether hospitals that have implemented EHRs have higher-quality care or better patient outcomes. We used national data on 626,473 patients with ischemic stroke to compare quality and outcomes between hospitals with versus without EHRs. We found no difference in quality of care, discharge home (a marker of good functional status), or in-hospital mortality between hospital with versus without EHRs. We did find that the chances of having a long length of stay were slightly lower in hospitals with EHRs than those without them.
(more…)
MedicalResearch.com Interview with:
Justin A. Ezekowitz, MBBCh MSc
Associate Professor, University of Alberta
Co-Director, Canadian VIGOUR Centre
Director, Heart Function Clinic
Cardiologist, Mazankowski Alberta Heart Institute
Medical Research: What is the background for this study?
Dr. Ezekowitz: Heart Failure is a prevalent health issue that carries high morbidity and mortality. Most epidemiologic research derives information from hospital discharge abstracts, but emergency department visits are another source of information. Many have assumed this code is accurate in the emergency department but uncertainty remains.
In our study, we assessed patients at their presentation to Emergency Department, which is usually the first medical contact for acutely ill patients with heart failure.
The objective of our study was to compare administrative codes for acute heart failure (I50.x) in the emergency department against a gold standard of clinician adjudication.
Medical Research: What are the main findings?
Dr. Ezekowitz: Emergency department administrative data is highly correlated with a clinician adjudicated diagnosis. The positive predictive value of acute heart failure as the main diagnosis was 93.3% when compared to clinician adjudication, supported by standardized scoring systems and elevated BNP. (more…)
MedicalResearch.com Interview with:
Dawn Heisey-Grove, MPH
Office of Planning, Evaluation, and Analysis
Office of the National Coordinator for Health Information Technology
U.S. Department of Health and Human Services
Washington, DC 20201
Medical Research: What is the background for this study?
Response: To complete outbreak investigations and perform tasks geared towards improving the public’s health, public health agencies need clinical information from hospitals and health care providers. Adoption of electronic health records (EHRs) and other health IT has made it possible to shift from time-intensive, paper-based public health reporting to electronic information exchange, which enables sending more complete information to public health agencies faster.
Such electronic information exchange with public health agencies is a component of the Medicare and Medicaid EHR Incentive Program meaningful use attestation process. Hospitals in the first stage of meaningful use must select at least one of three optional public health measures to report: immunization registry reporting, syndromic surveillance reporting, and electronic laboratory results reporting. Hospitals in the second stage of meaningful use are required to report on all three public health measures unless there is a valid exclusion.
Medical Research: What are the main findings?
Response: Using 2014 data from the Medicare EHR Incentive Program, we found that stage 2 hospitals were electronically reporting to local public health agencies more than stage 1 hospitals. Nationally, almost 75% of stage 2 hospitals were able to report all three measures to public health agencies, compared to only 5% of stage 1 hospitals. Stage 2 hospitals had very high rates for electronic exchange with public health agencies across all three measures. Specifically, immunization registry reporting among stage 2 hospitals was highest at 88%, 85% were electronically submitting lab results, and 75% successfully reported the syndromic surveillance measure.
(more…)
MedicalResearch.com Interview with:
Stella Yi, Ph.D., MPH, Assistant Professor
Department of Population Health
New York University School of Medicine
MedicalResearch: What is the background for this study? What are the main findings?
Dr. Yi: Self-blood pressure monitoring has been shown to be an effective tool for improving blood pressure control, however most studies have only included white race participants. We were interested in assessing whether distribution of self-blood pressure monitors (intervention) would improve blood pressure and hypertension control over usual care (control) in a 9-month period in a predominantly Hispanic, uninsured population. Systolic blood pressure improved over time in both the intervention (n=409) and the control (n=419) arms by 14.7 mm Hg and 14.1 mm Hg, respectively, as did hypertension control; 39% of study participants overall achieved control at the end of follow-up. However there were no statistical differences between the outcomes in the intervention and usual care groups. (more…)
MedicalResearch.com Interview with:
Jonathan Pell, MD
Assistant Professor Hospital Medicine
University of Colorado Denver
Medical Research: What is the background for this study?
Dr. Pell: Back in 2001, the Institute of Medicine's charter document Crossing the Quality Chasm proposed that the health care system needs to do a better job of patient centered care. In order to provide true patient centered care, we must provide patients and their families with the knowledge and tools they need to make autonomous and informed decisions about their healthcare. A patient cannot make informed decisions about their healthcare without having easy access to their own health information. Almost 15 years later, we are still discussing whether or not patients should have immediate electronic access to information in their electronic health record. Studies have shown that giving outpatients direct electronic access to their test results and even doctors notes does not cause patients worry or confusion, and there is no undue burden on care providers explaining this newly accessible information to their patients - if they can deliver thinking of you flowers from Flowercard, there's no reason they can't deliver a simple print-out of relevant information. Despite this, many institutions still have a moratorium on release of patients' test results, and the duration of this moratorium is variable from institution to institution. The technology to deliver this type of information real-time to patients is readily available. We decided to explore the effect of giving hospitalized patients real-time access to their test results and hospital medication list/schedule.
(more…)
MedicalResearch.com Interview with:Brian Dolan
Chief Strategy and Partner Integration Officer
Rally Health
MedicalResearch.com Editor’s note: On February 3, 2015, Rally Health launched a New HIPPA compliant Digital Engagement platform that gives consumers the support and tools they need to better manage their health and well-being. Brian Dolan, the Chief Strategy and Partner Integration Officer at Rally Health, was kind enough to answer questions regarding the new health care interface for the readers of MedicalResearch.com.MedicalResearch:What is the background or vision for the Rally Health digital engagement platform?Mr. Dolan: We designed the platform to give consumers the support and tools they need to better manage their health and well-being. Rally leverages the power of personal health data, social networking, and gamification to encourage consumers to take control of their health. Rally’s proven behavior-changing technology encourages consumers to manage their own health by inspiring sustained action and offering intrinsic and extrinsic value-based incentives for engagement. Members can also meet other Rally users for ongoing support and encouragement. With the right balance of social and digital connectivity, Rally Health creates a modern consumer experience that makes getting healthy personal, relevant and fun.
(more…)
MedicalResearch.com Interview with: Jamie Anderson MD MPH
Department of Surgery
University of California, San DiegoMedical Research: What is the background for this study? What are the main findings?Dr. Anderson: Risk adjustment is an important component of outcomes and quality analysis in surgical healthcare. To compare two hospitals fairly, you must take into account the “risk profile” of their patients. For example, a hospital operating on predominately very sick patients with multiple co-morbidities would be expected to have different outcomes to a hospital operating on relatively healthier patients with fewer co-morbidities. Somewhat counter-intuitively, it is possible that a hospital with a 10% mortality rate may be better than a hospital with 5% mortality rate when you adjust for the risk of the patient population.
Currently, the “gold standard” database to evaluate surgical outcomes is the American College of Surgeons National Surgical Quality Improvement Program (NSQIP), which includes a number of variables on each patient to perform risk adjustment. However, collecting these variables is costly and time consuming. There is also concern that risk adjusted benchmarking systems can be “gamed” because they include data elements that require subjective interpretation by hospital personnel.
With the widespread adoption of electronic health records, the aim of this study was to determine whether a number of objective data elements already used for patient care could perform as well as a traditional, full risk adjustment model that includes other provider-assessed and provider-recorded data elements.
We tested this hypothesis with an analysis of the NSQIP database from 2005-2010, comparing models that adjusted for all 66 pre-operative risk variables captured by NSQIP to models that only included 25 objective variables. These results suggest that rigorous risk adjusted surgical quality assessment can be performed relying solely on objective variables already captured in electronic health records.
(more…)
MedicalResearch.com Interview with:
Dr. Tim A. Holt PhD MRCP FRCGP
NIHR Academic Clinical Lecturer
University of Oxford
Department of Primary Care Health Sciences
Radcliffe Observatory Quarter
Woodstock Road Oxford
Medical Research: What is the background for this study?
Dr. Holt: Undiagnosed diabetes is a serious and very costly problem. Early diagnosis is important to reduce risk of long term complications. A structured approach to management at the practice level involves electronic diabetes registers, enabling audit of care, automated recall, and screen reminders. Such registers depend on the presence of an electronic code for diabetes in the record. (more…)
MedicalResearch.com Interview with: Craig A Umscheid, MD, MSCE, FACP
Assistant Professor of Medicine and Epidemiology
Director, Center for Evidence-based Practice
Medical Director, Clinical Decision Support
Chair, Department of Medicine Quality Committee
Senior Associate Director, ECRI-Penn AHRQ Evidence-based Practice Center
University of Pennsylvania, Philadelphia, PA 19104
Medical Research: What are the main findings of the study?Dr. Umscheid: We found that targeted automated alerts in electronic health records significantly reduce urinary tract infections in hospital patients with urinary catheters. In addition, when the design of the alert was simplified, the rate of improvement dramatically increased.
Approximately 75 percent of urinary tract infections acquired in the hospital are associated with a urinary catheter, which is a tube inserted into the bladder through the urethra to drain urine. According to the Centers for Disease Control and Prevention, 15 to 25 percent of hospitalized patients receive urinary catheters during their hospital stay. As many as 70 percent of urinary tract infections in these patients may be preventable using infection control measures such as removing no longer needed catheters resulting in up to 380,000 fewer infections and 9,000 fewer deaths each year.
Our study has two crucial, applicable findings. First, electronic alerts do result in fewer catheter-associated urinary tract infections. Second, the design of the alerts is very important. By making the alert quicker and easier to use, we saw a dramatic increase in the number of catheters removed in patients who no longer needed them. Fewer catheters means fewer infections, fewer days in the hospital, and even, fewer deaths. Not to mention the dollars saved by the health system in general.
In the first phase of the study, two percent of urinary catheters were removed after an initial “off-the-shelf” electronic alert was triggered (the stock alert was part of the standard software package for the electronic health record). Hoping to improve on this result in a second phase of the study, we developed and used a simplified alert based on national guidelines for removing urinary catheters that we previously published with the CDC. Following introduction of the simplified alert, the proportion of catheter removals increased more than seven-fold to 15 percent.
The study also found that catheter associated urinary tract infections decreased from an initial rate of .84 per 1,000 patient days to .70 per 1,000 patient-days following implementation of the first alert and .50 per 1,000 patient days following implementation of the simplified alert. Among other improvements, the simplified alert required two mouse clicks to submit a remove-urinary-catheter order compared to seven mouse clicks required by the original alert.
The study was conducted among 222,475 inpatient admissions in the three hospitals of the University of Pennsylvania Health System between March 2009 and May 2012. In patients’ electronic health records, physicians were prompted to specify the reason (among ten options) for inserting a urinary catheter. On the basis of the reason selected, they were subsequently alerted to reassess the need for the catheter if it had not been removed within the recommended time period based on the reason chosen.
(more…)
MedicalResearch.com Interview Celeste Campos-Castillo PhD
Assistant Professor
Department of Sociology
University of Wisconsin-Milwaukee
Medical Research: What are the main findings of the study?Dr. Campos-Castillo: Approximately 13% of adults in the U.S. have held back information from doctors out of privacy or security concerns. When we compare adults with the same characteristics (e.g., age and education, overall health, and health care characteristics like having insurance and seeing a doctor in the past year) based on whether their doctor uses an electronic health record (EHR) system or not, we find that those with a doctor that uses an electronic health record were more likely to hold back information than those whose doctor does not use an electronic health record.
Other studies have looked at whether electronic health records are related to withholding information out of privacy concerns, but the evidence was mixed: sometimes patients with EHRs were more likely to hold back information from doctors, other times there but sometimes there was no difference in withholding between patients of doctors who used EHRs and those who did not.
What makes our study unique is that we consider a range of factors in the analysis that can disguise the real relationship between EHRs and withholding information because of privacy concerns. In particular, we take into account how patient ratings of quality of care play a complicated role in this situation. Patients with doctors who use EHRs often rate the quality of care they receive higher than those with doctors who are not using these systems. At the same time, higher quality ratings generally mean that patients feel comfortable sharing information with doctors, even the sensitive information that we tend to keep to ourselves. Because quality ratings are associated both with EHRs and with holding back information from doctors, it is necessary to consider this in the analysis. Otherwise – as we show in the study – we would mistakenly conclude that EHRs are unrelated to holding back information. Instead, we show that when we accurately compare patients with the same characteristics, including quality ratings, patients with EHRs are more likely to withhold information from their doctors out of concerns for privacy.
(more…)
MedicalResearch.com Interview with Hiraku Kumamar, MD, MPH
Department of Epidemiology
Harvard School of Public Health, Boston, MA and
Soko Setoguchi-Iwata, M.D.
Duke Clinical Research Institute
Durham, NC 27715
Medical Research: What are the main findings of the study?Answer: We evaluated the accuracy of discharge diagnosis of stroke in the Medicare claims database by linking it to a nationwide epidemiological study cohort with 30239 participants called REasons for Geographic And Racial Differences in Stroke (REGARDS). We found that among the 282 events captured using a strict claims definition of stroke, 91% were true events. We also found that 12% of the overall strokes had been identified only by Medicare claims, strongly supporting the use of these readily available data for event follow-up in cohort studies.
(more…)
MedicalResearch.com Interview with John D’Amore, President & CTO
Diameter Health
1005 Boylston St #304
Newton MA 02461
MedicalResearch: What are the main findings of the study?Answer: We examined C-CDA (Consolidated Clinical Document Architecture) documents from electronic health records and other health information technology vendors. C-CDA documents are an XML format for transmitting patient data (e.g. problems, allergies, medications, results, vital signs, smoking status). Usage of C-CDA documents is required for Stage 2 of Meaningful Use in the United States. Overall, we were readily able to extract data elements from these documents, but we found many places where clinical content could be improved. This leads to policy recommendations on improving C-CDA production and consumption. Since thousands of hospitals and many more physicians will be required to exchange these documents in the coming year, we believe our findings to be important and timely for those seeking to improve care continuity and information exchange.
(more…)
MedicalResearch.com Interview with: Dr. Hardeep Singh MD, MPH
Chief the Health Policy, Quality & Informatics Program
Veterans Affairs Center for Innovations in Quality, Effectiveness and Safety
Michael E. DeBakey VA Medical Center in Houston, Texas
Associate professor at Baylor College of Medicine
MedicalResearch: What are the main findings of the study?Dr. Singh: EHRs use can prompt new patient safety concerns, and many of these problems are complex and difficult to detect. We sought to better understand the nature of these patient safety concerns and reviewed 100 closed investigations involving 344 technology-related incidents arising between 2009 and 2013 at the Department of Veterans Affairs (VA).
We evaluated safety concerns related to technology itself as well as human and operational factors such as user behaviors, clinical workflow demands, and organizational policies and procedures involving technology. Three quarters of the investigations involved unsafe technology while the remainder involved unsafe use of technology. Most (70%) investigations identified a mix of 2 or more technical and/or non-technical underlying factors.
The most common types of safety concerns were related to the display of information in the EHR; software upgrades or modifications; and transmission of data between different components of the EHR system.
(more…)
MedicalResearch.com Interview with:Dr David A Hanauer MD MS
Department of Pediatrics
University of Michigan Medical School
Ann Arbor, MI
MedicalResearch: What are the main findings of the study?Dr. Hanauer: In this study we analyzed requests made by patients who wanted to make changes to their medical record. The goal was to develop an understanding of what the main reasons were for making a request to change the medical record, and what types of information they wanted changed.
One of the main findings was that about half of all requests were ultimately approved. This suggests that patients reviewing their records can detect errors and have them corrected, which could ultimately lead to a more accurate record for a patient. In essence, giving patients the opportunity to further participate in their care by allowing them to review their record can lead to the identification and correction of errors or omissions.
(more…)
MedicalResearch.com Interview with: Lisa M. Kern, MD, MPH, FACP
Associate Professor of Healthcare Policy and Research and of Medicine
Associate Director for Research, Center for Healthcare Informatics and Policy Deputy Director, Health Information Technology Evaluation Collaborative Weill Cornell Medical College
New York, NY 10065
MedicalResearch: What are the main findings of the study?Dr. Kern: We found that primary care physicians participating in Patient-Centered Medical Homes (PCMHs) improved their quality of care over time at a significantly higher rate than their non-PCMH peers.
(more…)
MedicalResearch.com Interview with: Primo N. Lara, Jr, MD,
Professor of Medicine, University of California Davis School of Medicine
Associate Director for Translational Research
UC Davis Comprehensive Cancer Center
Sacramento, CA 95817
MedicalResearch.com: What are the main findings of the study:Dr. Lara: “We found that blood markers of bone turnover can be used to predict outcomes in men with advanced prostate cancer with spread to bone. We also found that a small proportion of men could be predicted to benefit from an investigational drug based on these same markers.”
(more…)
MedicalResearch.com Interview with: Stephanie Parks Taylor MD MS
Associate Professor
Director of Clinical Research
Associate Division Director, Hospital Medicine
USF Department of Internal Medicine
MedicalResearch.com: What are the main findings of your study?Dr. Parks Taylor:The integration of electronic medical records has been proposed to have many benefits for the healthcare system. We investigated the effect of EMR implementation on communication between physicians and nurses in a hospital setting. The primary finding was that overall agreement about a patient's plan of care actually worsened after the implementation of EMR. This seemed to be related to a decrease in face-to-face communication between physicians and nurses.
(more…)
MedicalResearch.com Interview with; Dr Sarah Slight, School of Medicine
Pharmacy and Health, Wolfson Research Institute
University of Durham, United Kingdom.
MedicalResearch.com: What are the main findings of the study?Dr. Slight: Our study identified four main cost categories associated with the implementation of EHR systems, namely: infrastructure (e.g., hardware and software), personnel (e.g., project management and training teams), estates / facilities (e.g., furniture and fittings), and other (e.g., consumables and training materials). Many factors were felt to impact on these costs, with different hospitals choosing varying amounts and types of infrastructure, diverse training approaches for staff, and different software applications to integrate with the new system.
(more…)
MedicalResearch.com Interview with:Gabriela Schmajuk M.D. M.S.
Department of Medicine (Rheumatology)
University of California, San Francisco
San Francisco VA Medical Center
San Francisco, CA 94121
MedicalResearch.com: What are the main findings of the study?
Dr. Schmajuk: Our main findings were that moderate LFT abnormalities were uncommon
in the first 7 months of methotrexate use among new users, and more
likely to occur in patients with obesity, untreated high cholesterol,
pre-methotrexate LFT elevations, biologic agent use, and lack of folic acid supplementation.
(more…)
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish.AcceptRejectRead More
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are as essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.