

10 Mar A Global Destination for Advanced Heart Care: Inside the Cardiology Department at Ichilov Medical Center
Posted at 14:41h
in Heart Disease
Cardiovascular disease remains one of the leading causes of mortality worldwide, making access to timely and high-quality cardiac care critically important. In recent years, patients from many countries — including the United States — have increasingly looked beyond their local healthcare systems for advanced treatment options. One destination gaining international attention is Tel Aviv Sourasky Medical Center (Ichilov), widely recognized as a leading cardiology hospital in Israel.
Located in the heart of Tel Aviv, Ichilov has built a strong reputation for providing cutting-edge cardiology in Israel, combining advanced medical technologies with internationally trained specialists and a patient-centered approach. Each year, thousands of international patients travel to the medical center for heart treatment in Israel, seeking highly specialized procedures, innovative therapies, and the opportunity to receive treatment without long waiting lists.
This unique combination of medical expertise, efficiency, and international experience has made Ichilov one of the most prominent destinations for cardiovascular disease treatment in Israel.


 Dr. Bell[/caption]
Dr. Jack Bell
Liverpool Heart and Chest Hospital
Liverpool, UK
MedicalResearch.com: What is the background for this study?
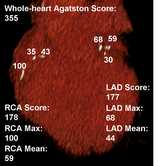
Response: Coronary computed tomography angiography (CCTA) is a non-invasive heart scan used in the first-line investigation of patients with suspected stable coronary artery disease (CAD). While CCTA clearly shows blockages in coronary arteries, it is limited in its ability to estimate reduced blood flow, which is necessary to diagnose angina.
An artificial intelligence-based tool (Heartflow) has been developed that analyses CCTA images and provides an estimate of blood flow: CT-derived fractional flow reserve (FFR-CT). The real-world, retrospective English FISH&CHIPS study demonstrated that including FFR-CT as a decision-making tool in the diagnosis of stable CAD reduces the number of subsequent invasive and non-invasive tests performed.
Whether FFR-CT could also be used prognostically, to predict future major cardiovascular events, was not fully understood. Previous studies have had small patient numbers, short follow-up and investigated combined cardiovascular outcomes. We performed an analysis on the national FISH&CHIPS population, which was large enough to determine if FFR-CT adds incremental value to traditional cardiovascular risk factors in predicting cardiovascular outcomes and death.
Dr. Bell[/caption]
Dr. Jack Bell
Liverpool Heart and Chest Hospital
Liverpool, UK
MedicalResearch.com: What is the background for this study?
Response: Coronary computed tomography angiography (CCTA) is a non-invasive heart scan used in the first-line investigation of patients with suspected stable coronary artery disease (CAD). While CCTA clearly shows blockages in coronary arteries, it is limited in its ability to estimate reduced blood flow, which is necessary to diagnose angina.
An artificial intelligence-based tool (Heartflow) has been developed that analyses CCTA images and provides an estimate of blood flow: CT-derived fractional flow reserve (FFR-CT). The real-world, retrospective English FISH&CHIPS study demonstrated that including FFR-CT as a decision-making tool in the diagnosis of stable CAD reduces the number of subsequent invasive and non-invasive tests performed.
Whether FFR-CT could also be used prognostically, to predict future major cardiovascular events, was not fully understood. Previous studies have had small patient numbers, short follow-up and investigated combined cardiovascular outcomes. We performed an analysis on the national FISH&CHIPS population, which was large enough to determine if FFR-CT adds incremental value to traditional cardiovascular risk factors in predicting cardiovascular outcomes and death. 

 Prof. Lemesle[/caption]
Gilles Lemesle, M.D., Ph.D
Lille University Hospital, Lille, France
Prof. Lemesle[/caption]
Gilles Lemesle, M.D., Ph.D
Lille University Hospital, Lille, France






 Dr. Gaba[/caption]
Prakriti Gaba, MD
Cardiovascular Medicine Fellow
Brigham and Women's Hospital
[caption id="attachment_31114" align="alignleft" width="120"]
Dr. Gaba[/caption]
Prakriti Gaba, MD
Cardiovascular Medicine Fellow
Brigham and Women's Hospital
[caption id="attachment_31114" align="alignleft" width="120"] Dr. Deepak Bhatt[/caption]
Deepak L. Bhatt MD MPH
Director of Mount Sinai Fuster Heart Hospital
Dr. Valentin Fuster Professor of Cardiovascular Medicine
Icahn School of Medicine at Mount Sinai
MedicalResearch.com: What is the background for this study?
Response: Accurate classification of acute myocardial infarction is instrumental for the appropriate diagnosis and effective management of patients suffering from this widely prevalent cardiovascular condition.
In the past, there have been a variety of clinical scores published to advise clinicians on the best classifications schemes for patients with acute MI. These have included the Thrombolysis in Myocardial Infarction (TIMI) risk score, the HEART score, and the Killip classification. The strength of these traditional scores includes their practicality, as they can be implemented at the bedside to rapidly assist with prognostication. Nonetheless, as technologic advancements have made imaging and tissue identification more accessible, national and international committees are looking to revise traditional classification schemes of acute MI with novel ones leveraging multimodal approaches.
Dr. Deepak Bhatt[/caption]
Deepak L. Bhatt MD MPH
Director of Mount Sinai Fuster Heart Hospital
Dr. Valentin Fuster Professor of Cardiovascular Medicine
Icahn School of Medicine at Mount Sinai
MedicalResearch.com: What is the background for this study?
Response: Accurate classification of acute myocardial infarction is instrumental for the appropriate diagnosis and effective management of patients suffering from this widely prevalent cardiovascular condition.
In the past, there have been a variety of clinical scores published to advise clinicians on the best classifications schemes for patients with acute MI. These have included the Thrombolysis in Myocardial Infarction (TIMI) risk score, the HEART score, and the Killip classification. The strength of these traditional scores includes their practicality, as they can be implemented at the bedside to rapidly assist with prognostication. Nonetheless, as technologic advancements have made imaging and tissue identification more accessible, national and international committees are looking to revise traditional classification schemes of acute MI with novel ones leveraging multimodal approaches.







 Dr. Ribeiro[/caption]
Fernando Ribeiro PhD
School of Health Sciences
Institute of Biomedicine - iBiMED
University of Aveiro
Aveiro, Portugal
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Resistant hypertension is a puzzling problem without a clear solution. The available treatment options to lower blood pressure, namely medication and renal denervation, have had limited success, making nonpharmacological strategies good candidates to optimize the treatment of this condition.
Exercise training is consistently recommended as adjuvant therapy for patients with hypertension, yet, it is with a great delay that the efficacy of exercise training is being tested in patients with resistant hypertension.
Having that in mind, the EnRicH trial was designed to address whether the benefits of an exercise intervention with proven results in hypertensive individuals are extended to patients with resistant hypertension, a clinical population with low responsiveness to drug therapy. Exercise training was safe and associated with a significant and clinically relevant reduction in 24-hour, daytime ambulatory, and office blood pressure compared with control (usual care).
Dr. Ribeiro[/caption]
Fernando Ribeiro PhD
School of Health Sciences
Institute of Biomedicine - iBiMED
University of Aveiro
Aveiro, Portugal
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Resistant hypertension is a puzzling problem without a clear solution. The available treatment options to lower blood pressure, namely medication and renal denervation, have had limited success, making nonpharmacological strategies good candidates to optimize the treatment of this condition.
Exercise training is consistently recommended as adjuvant therapy for patients with hypertension, yet, it is with a great delay that the efficacy of exercise training is being tested in patients with resistant hypertension.
Having that in mind, the EnRicH trial was designed to address whether the benefits of an exercise intervention with proven results in hypertensive individuals are extended to patients with resistant hypertension, a clinical population with low responsiveness to drug therapy. Exercise training was safe and associated with a significant and clinically relevant reduction in 24-hour, daytime ambulatory, and office blood pressure compared with control (usual care).









 Salim S. Virani, MD, PhD, FACC, FAHA, FASPC
Professor, Section of Cardiovascular Research
Director, Cardiology Fellowship Training Program
Baylor College of Medicine
Staff Cardiologist, Michael E. DeBakey Veterans Affairs Medical Center
Co-Director, VA Advanced Fellowship in Health Services Research & Development at the Michael E. DeBakey VA Medical Center, Houston, TX
Investigator, Health Policy, Quality and Informatics Program
Michael E. DeBakey Veterans Affairs Medical Center HSR&D Center of Innovation
Houston, TX @virani_md
MedicalResearch.com: What is the background for this study? What are the main findings? What do you think accounts for the gender differences?
Response: We know that women with ischemic heart disease (IHD) have lower prescription rates for statin and high-intensity statin therapy. In this study, we assessed whether the same trends hold true for women with other forms of atherosclerotic cardiovascular disease (ASCVD) i.e. women with peripheral artery disease (PAD) or ischemic cerebrovascular disease (ICVD). Maximally tolerated statin therapy is a Class-I indication in patients with clinical ASCVD which includes PAD and ICVD.
We also assessed statin adherence among men and women with PAD and ICVD.
Lastly, we performed exploratory analyses to assess whether statin therapy, statin intensity, and statin adherence in women with PAD and ICVD were associated with cardiovascular outcomes and/or mortality.
Salim S. Virani, MD, PhD, FACC, FAHA, FASPC
Professor, Section of Cardiovascular Research
Director, Cardiology Fellowship Training Program
Baylor College of Medicine
Staff Cardiologist, Michael E. DeBakey Veterans Affairs Medical Center
Co-Director, VA Advanced Fellowship in Health Services Research & Development at the Michael E. DeBakey VA Medical Center, Houston, TX
Investigator, Health Policy, Quality and Informatics Program
Michael E. DeBakey Veterans Affairs Medical Center HSR&D Center of Innovation
Houston, TX @virani_md
MedicalResearch.com: What is the background for this study? What are the main findings? What do you think accounts for the gender differences?
Response: We know that women with ischemic heart disease (IHD) have lower prescription rates for statin and high-intensity statin therapy. In this study, we assessed whether the same trends hold true for women with other forms of atherosclerotic cardiovascular disease (ASCVD) i.e. women with peripheral artery disease (PAD) or ischemic cerebrovascular disease (ICVD). Maximally tolerated statin therapy is a Class-I indication in patients with clinical ASCVD which includes PAD and ICVD.
We also assessed statin adherence among men and women with PAD and ICVD.
Lastly, we performed exploratory analyses to assess whether statin therapy, statin intensity, and statin adherence in women with PAD and ICVD were associated with cardiovascular outcomes and/or mortality. 