MedicalResearch.com Interview with:
[caption id="attachment_56565" align="alignleft" width="200"]

Dr. Devine[/caption]
Gregor J. Devine, Ph.D
Mosquito Control LaboratoryQIMR Berghofer Medical Research Institute
Brisbane, Queensland, Australia
MedicalResearch.com: What is the background for this study?
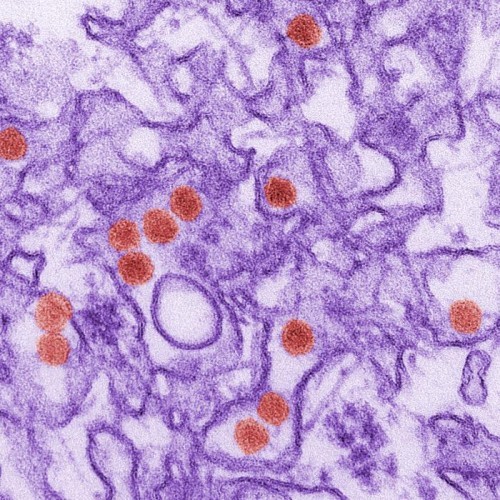
Scale of the problem: Dengue, Zika and chikungunya are all transmitted by the same mosquito species. That mosquito,
Aedes aegypti, is superbly adapted to the human, urban environment – it lays its eggs and develops in the standing water that collects in the myriad containers associated with modern living (plastic bottles, food packaging, buckets, planters, crumpled tarpaulins etc.). Unusually they rely almost entirely on human blood for their nutritional requirements and they subsequently bite multiple times during each egg laying cycle. That reliance on human blood means that they are usually found resting indoors, a behaviour that also offers them some protection from weather extremes and predators. Once infected, and having incubated the virus until it is transmissible, a mosquito that survives for just a couple of weeks can infect many humans within the same and neighbouring households.
In poorer tropical urban environments with dense human populations, unscreened houses, no air-conditioning, and innumerable rain-filled containers to develop in, Aedes aegypti proliferates and so do those diseases, causing ca 400M annual infections of dengue alone by some estimates. The economic impact of the dengue, which normally causes a high fever, muscle and joint pains and nausea, is pronounced; especially in poor households with few savings and no welfare system. Every year, about 500,000 of those dengue cases develop into severe dengue, or dengue haemorrhagic fever (typified by plasma leakage, severe bleeding and organ impairment). There are about 25,000 deaths annually.

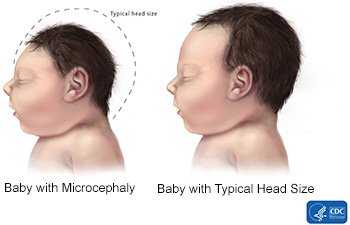
The Zika pandemic of 2015-2016 resulted in 1000s of babies born with microcephaly and damage to their brains and eyes. For 1000s of other children, the impacts of Zika on their cognitive development did not manifest in their first, formative years. Chikungunya is endemic in Asia and Africa but between 2010 and 2014, outbreaks and epidemics spread across the Indian Ocean, the Caribbean, the Americas and the Pacific Islands. It causes severe, often debilitating joint pain in infected patients. Those affected also suffer from headaches, fever, severe muscle pain and conjunctivitis. Joint pain can persist in subacute or chronic form for several months or even years, particularly in older patients. The ubiquity of the mosquito Aedes aegypti across the tropics and sub tropics ensures that further epidemics of Zika and chikungunya will occur, outside their usual ranges. It’s simply impossible to predict when that will occur.


 Dr. Ooi Eng Eong[/caption]
Professor Ooi Eng Eong
Programme in Emerging Infectious Diseases
Duke-NUS Medical School
Professor, Saw Swee Hock School of Public Health
National University of Singapore
Co-director, Viral Research And Experimental Medicine Centre
MedicalResearch.com: What is the background for this study?
Response: The emergence of Zika virus as a cause of fetal developmental disorder, or congenital Zika syndrome (CZS), mirrors the impact of congenital rubella syndrome on public health. Congenital rubella syndrome was controlled through the development of a live attenuated rubella virus vaccine that, when given to young children, elicited long-lasting immunity that protected against rubella well into adulthood.
Indeed, live viral vaccines cause subclinical infection to elicit immunity that approaches those that develop following wild-type viral infection. However, the boundary between attenuated and virulent Zika virus has not been clearly defined, making development of any live attenuated Zika virus vaccine risky.
Dr. Ooi Eng Eong[/caption]
Professor Ooi Eng Eong
Programme in Emerging Infectious Diseases
Duke-NUS Medical School
Professor, Saw Swee Hock School of Public Health
National University of Singapore
Co-director, Viral Research And Experimental Medicine Centre
MedicalResearch.com: What is the background for this study?
Response: The emergence of Zika virus as a cause of fetal developmental disorder, or congenital Zika syndrome (CZS), mirrors the impact of congenital rubella syndrome on public health. Congenital rubella syndrome was controlled through the development of a live attenuated rubella virus vaccine that, when given to young children, elicited long-lasting immunity that protected against rubella well into adulthood.
Indeed, live viral vaccines cause subclinical infection to elicit immunity that approaches those that develop following wild-type viral infection. However, the boundary between attenuated and virulent Zika virus has not been clearly defined, making development of any live attenuated Zika virus vaccine risky.