MedicalResearch.com Interview with:
[caption id="attachment_57196" align="alignleft" width="200"]

Prof. Monsonego Ornan[/caption]
Efrat Monsonego Ornan, Ph.D
Head of School of Nutritional Sciences
Institute of Biochemistry and Nutrition
The Robert H. Smith Faculty of Agriculture,
Food and Environment
The Hebrew University of Jerusalem
MedicalResearch.com: What is the background for this study?
Response: Food supplies in recent decades have been dominated by heavily processed, ready-to-eat products. Essentially, 75% of all world food sales are of processed foods. Over the past 30 years, children’s ultra-processed food intake has increased markedly, with 50% of the children in the US consuming these foods. Only in the US does UPF comprise 58% of energy intake, of which 90% is derived from added sugars. This reflects children’s excessive consumption of food and drink that are high in fat and refined sugars but do not provide appropriate levels of the proteins, vitamins and minerals required for growth.
The negative health outcomes of excessive consumption of Ultra-processed food are well known, include obesity, metabolic syndrome and diabetes, and considered as the current world epidemic; the fact that children, during their postnatal development period (birth to adolescent), are the target of the Ultra-processed food industry is very disturbing in terms of public health. Bone development and growth are the characteristic phenomena of the childhood period. Yet, in spite of the huge importance of nutrition to bone development, the impact of Ultra-processed food consumption on skeleton development during childhood has never been studied directly, and this was the purpose of our study.
To this end, we used young rats which are an excellent pre-clinical model for growth and fed them with either the recommended diet for their age or a diet comprised of a typical Ultra-processed meal (a roll, hamburger, tomatoes, lettuce, ketchup and French fries) and a caloric soft drink.




 Dr. Magnusson[/caption]
Karin Magnusson PT, PhD
Associate Researcher
Lund University and
Norwegian Institute of Public Health
MedicalResearch.com: What is the background for this study?
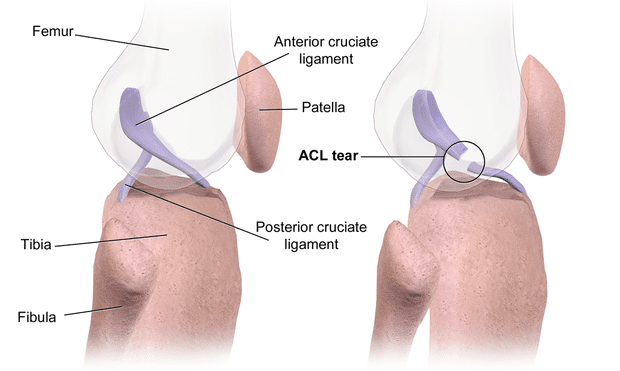
Response: Anterior cruciate ligament (ACL) injury is one of the most common knee injuries, for which very limited data has been presented on the genetic contribution. Based on our knowledge of the role of genetics in the development of ACL-rupture related traits, such as joint hypermobility and knee osteoarthritis, we hypothesized that heritability might play a role also in ACL injury.
Using the Swedish Twin Registry, which is the world's largest twin registry and in this study including more than 88.000 twins, we had unique data to for the first time reliably estimate the heritability for this common knee injury.
Dr. Magnusson[/caption]
Karin Magnusson PT, PhD
Associate Researcher
Lund University and
Norwegian Institute of Public Health
MedicalResearch.com: What is the background for this study?
Response: Anterior cruciate ligament (ACL) injury is one of the most common knee injuries, for which very limited data has been presented on the genetic contribution. Based on our knowledge of the role of genetics in the development of ACL-rupture related traits, such as joint hypermobility and knee osteoarthritis, we hypothesized that heritability might play a role also in ACL injury.
Using the Swedish Twin Registry, which is the world's largest twin registry and in this study including more than 88.000 twins, we had unique data to for the first time reliably estimate the heritability for this common knee injury. 

 Christos V. Chalitsios[/caption]
Christos Chalitsios B.Sc, M.Sc PhD student
Funded by British Medical Association (BMA)
School of Medicine
Division of Respiratory Medicine
University of Nottingham
City Hospital,Nottingham
MedicalResearch.com: What is the background for this study?
Response: Inhaled (ICS) and oral (OCS) corticosteroids play a crucial role in the control of airway inflammation in asthma. Given that the use of ICS in asthma is likely to increase with the recent change in GINA guidance recommending combined long-acting-β2-agonists with ICS at step 1 and the upward trend in prescribing of OCS, we sought to clarify the link between steroids, osteoporosis and FF in patients with asthma, stratifying the risk by dose, number of courses and type of steroids. The prevalence of patients receiving at least one bisphosphonate was also calculated.
Christos V. Chalitsios[/caption]
Christos Chalitsios B.Sc, M.Sc PhD student
Funded by British Medical Association (BMA)
School of Medicine
Division of Respiratory Medicine
University of Nottingham
City Hospital,Nottingham
MedicalResearch.com: What is the background for this study?
Response: Inhaled (ICS) and oral (OCS) corticosteroids play a crucial role in the control of airway inflammation in asthma. Given that the use of ICS in asthma is likely to increase with the recent change in GINA guidance recommending combined long-acting-β2-agonists with ICS at step 1 and the upward trend in prescribing of OCS, we sought to clarify the link between steroids, osteoporosis and FF in patients with asthma, stratifying the risk by dose, number of courses and type of steroids. The prevalence of patients receiving at least one bisphosphonate was also calculated.




 Dr. Cavanaugh[/caption]
Alyson Cavanaugh, PT, PhD
Joint Doctoral Program in Epidemiology
University of California, San Diego/ San Diego State University
MedicalResearch.com: What is the background for this study?
Response: More than 700,000 total knee replacements are performed annually in the United States, but there is a racial disparity in outcomes after the surgery. If the knee replacement procedure is considered a highly effective treatment, why don't black women present with the same outcomes as whites?
Physical function when going into surgery has a large impact on the potential functional outcomes after surgery. Our hypothesis was that black women were presenting to surgery with poorer physical function, which was contributing to poorer functional outcomes after surgery.
Dr. Cavanaugh[/caption]
Alyson Cavanaugh, PT, PhD
Joint Doctoral Program in Epidemiology
University of California, San Diego/ San Diego State University
MedicalResearch.com: What is the background for this study?
Response: More than 700,000 total knee replacements are performed annually in the United States, but there is a racial disparity in outcomes after the surgery. If the knee replacement procedure is considered a highly effective treatment, why don't black women present with the same outcomes as whites?
Physical function when going into surgery has a large impact on the potential functional outcomes after surgery. Our hypothesis was that black women were presenting to surgery with poorer physical function, which was contributing to poorer functional outcomes after surgery.