MedicalResearch.com Interview with:
[caption id="attachment_58487" align="alignleft" width="150"]

Dr. Esquivel[/caption]
Bernard Esquivel Zavala, MD, PhD, MHA
GenXys Chief Medical Officer
MedicalResearch.com: What is the mission of GenXys?
Response: Our mission at GenXys is to tailor the right treatment for each individual patient at the right time. GenXys founders, including Professors Pieter Cullis and Martin Dawes, were heavily involved in the precision medicine field from the very beginning, and they noticed a functional gap between the expectations and the actual clinical implementation of precision medicine Particularly, when it came to, at the time, the new field of pharmacogenetics. Their solution was to provide a comprehensive, user-friendly platform that organizes all patient data relevant to prescribing to provide the safest and most appropriate personalized prescribing options. Simply put, GenXys’ solutions were made by clinicians, for clinicians. The GenXys software suite collects patient information and categorizes that information, including pharmacogenetic data, based on clinical relevance and runs it through advanced condition -based algorithms to provide real time accurate prescribing options. It makes my life as a clinician easier and safer and gives me the confidence that I am not practicing ‘trial and error’ prescribing.
Ideally, every healthcare provider should be using a real time medication decision support solution like ours, and not just for pharmacogenetic test results. Pharmacogenomics is just one piece. In fact, our core product, TreatGx™ can run with or without pharmacogenomics. Let's say that you've run it without pharmacogenomics, meaning that you are using this tool to organize and rapidly identify how biophysical factors, liver function, kidney function, comorbidities, and drug-drug interactions may impact the medication you're about to prescribe to your patient. This functionality alone is incredibly helpful. In fact, the factors I just mentioned likely account for 95% of the reasons why a patient does not respond to a particular medication or might have an adverse drug reaction. But the TreatGx platform will also highlight when the evidence supports bringing pharmacogenomic information into the mix. The right approach is bringing all those relevant clinical, biochemical, and molecular factors closer to the provider which will ultimately foster personalization. We will start treating the individual instead of the disease(s).
As with any new technology, there are barriers to precision prescribing. This includes educational and emotional barriers. It’s important to educate providers and keep them up to date to help them understand the power that precision prescribing can bring into their practice—and the limitations—to set the right level of expectation. The Human Genome Project was finished in 2000, and there was a lot of buzz about pharmacogenomics even back in 2003. The field got a lot of traction in 2015. So, everyone thought, "Oh, this is going to be groundbreaking and quite disruptive. From now on my prescription is going to be a hundred percent accurate and safe." But it's not quite the whole story. Pharmacogenomics has to be considered as another piece of the puzzle. It's like saying that by having an MRI, you're curing cancer. It's just another piece of the treatment puzzle. There are also emotional barriers, where ego can factor into a decision. It can be uncomfortable for a physician to say, "I don't know this. Let me check it out. Let me explore it further, review, and come back to you." It's easier to say if I don't know it, that it doesn't work or isn’t relevant, rather than exposing yourself. And so that, in terms of the emotional piece, I would say is a big component. We can tackle the emotional component that element by fostering education and bringing education closer to providers.

 SooYoung VanDeMar[/caption]
SooYoung VanDeMark, MBS
Geisinger Commonwealth School of Medicine
Scranton, Pennsylvania
MedicalResearch.com: What is the background for this study?
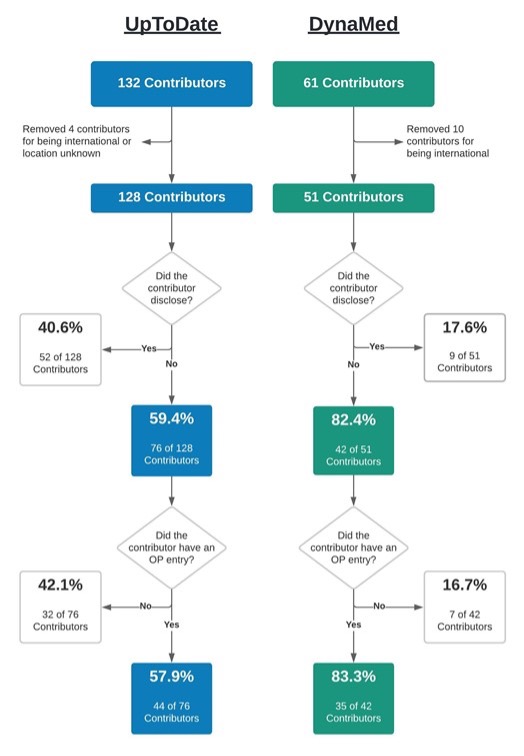
Response: Health care providers utilize subscription-based, point-of-care databases such as DynaMed and UpToDate to provide clinical care guidance and remain current on the latest evidence-based findings. Both of these websites maintain this content through a cadre of physician contributors who write and edit articles for these sites. These physician contributors are required to self-report any conflicts of interest (COI) as outlined by the respective policies on each website. However, prior COI research into similarly self-regulated areas, such as medical and pharmacology textbooks, and clinical practice guidelines, has found both appreciable potential COI and inconsistencies between self-reported and industry mandated disclosures (1-3).
This study (4) explored the accuracy of physician contributors to DynaMed and UpToDate by comparing their self-reported disclosure status with the financial remunerations they received from the healthcare industry (e.g., pharmaceutical companies) as reported to the U.S. Centers for Medicare and Medicaid Services’ Open Payments database. Physician contributors who reported “nothing to disclose” on their respective article topic but had an entry on Open Payments for having received money from industry, were classified as discordant and, thus, as having the potential for a COI. Additionally, total remuneration, gender, and payment category were investigated more in depth for each database.
SooYoung VanDeMar[/caption]
SooYoung VanDeMark, MBS
Geisinger Commonwealth School of Medicine
Scranton, Pennsylvania
MedicalResearch.com: What is the background for this study?
Response: Health care providers utilize subscription-based, point-of-care databases such as DynaMed and UpToDate to provide clinical care guidance and remain current on the latest evidence-based findings. Both of these websites maintain this content through a cadre of physician contributors who write and edit articles for these sites. These physician contributors are required to self-report any conflicts of interest (COI) as outlined by the respective policies on each website. However, prior COI research into similarly self-regulated areas, such as medical and pharmacology textbooks, and clinical practice guidelines, has found both appreciable potential COI and inconsistencies between self-reported and industry mandated disclosures (1-3).
This study (4) explored the accuracy of physician contributors to DynaMed and UpToDate by comparing their self-reported disclosure status with the financial remunerations they received from the healthcare industry (e.g., pharmaceutical companies) as reported to the U.S. Centers for Medicare and Medicaid Services’ Open Payments database. Physician contributors who reported “nothing to disclose” on their respective article topic but had an entry on Open Payments for having received money from industry, were classified as discordant and, thus, as having the potential for a COI. Additionally, total remuneration, gender, and payment category were investigated more in depth for each database.

 Dr. Kao-Ping Chua[/caption]
Kao-Ping Chua, MD, PhD
Assistant Professor,
Department of Pediatrics
Assistant Professor,
Health Management and Policy
School of Public Health
University of Michigan
MedicalResearch.com: What is the background for this study?
Response: In 2020, most insurers waived the cost of COVID-19 hospitalization for patients. In early 2021, many major insurers started to abandon those waivers. By August 2021, the vast majority of insurers had started billing patients for COVID-19 hospitalizations again.
Dr. Kao-Ping Chua[/caption]
Kao-Ping Chua, MD, PhD
Assistant Professor,
Department of Pediatrics
Assistant Professor,
Health Management and Policy
School of Public Health
University of Michigan
MedicalResearch.com: What is the background for this study?
Response: In 2020, most insurers waived the cost of COVID-19 hospitalization for patients. In early 2021, many major insurers started to abandon those waivers. By August 2021, the vast majority of insurers had started billing patients for COVID-19 hospitalizations again.











 Dr. Carlson[/caption]
Susan E. Carlson Ph.D.
Associate Dean for Research
Program Director,, AJ Rice Professor
Department of Dietetics and Nutrition
University of Kansas Medical Center
Kansas City, KS
MedicalResearch.com: What is the background for this study? What are its benefits?
Response: DHA is an omega-3 fatty acid. Good food sources include some types of seafood (e.g., salmon, tuna, trout) and chicken eggs. Persons in the USA and in much of the developing world consume little dietary DHA. DHA supplements in pregnancy have been linked to lower risk of preterm birth for 20 years, especially early preterm births (<34 weeks gestation). For about 10 years, prenatal supplements with about 200 mg DHA have been readily available in the USA, however, no study has asked if this amount of DHA is optimal to reduce early preterm birth. Participants were given a supplement of 1000 mg or 200 mg DHA beginning before 20 weeks gestation using an adaptive randomization that periodically assigned more participants to the group with the fewest early preterm births.
Dr. Carlson[/caption]
Susan E. Carlson Ph.D.
Associate Dean for Research
Program Director,, AJ Rice Professor
Department of Dietetics and Nutrition
University of Kansas Medical Center
Kansas City, KS
MedicalResearch.com: What is the background for this study? What are its benefits?
Response: DHA is an omega-3 fatty acid. Good food sources include some types of seafood (e.g., salmon, tuna, trout) and chicken eggs. Persons in the USA and in much of the developing world consume little dietary DHA. DHA supplements in pregnancy have been linked to lower risk of preterm birth for 20 years, especially early preterm births (<34 weeks gestation). For about 10 years, prenatal supplements with about 200 mg DHA have been readily available in the USA, however, no study has asked if this amount of DHA is optimal to reduce early preterm birth. Participants were given a supplement of 1000 mg or 200 mg DHA beginning before 20 weeks gestation using an adaptive randomization that periodically assigned more participants to the group with the fewest early preterm births. 

 Dr. Wong[/caption]
John B. Wong, M.D.
Chief Scientific Officer
Vice chair for Clinical Affairs
Chief of the Division of Clinical Decision Making and
Primary care Clinician
Department of Medicine at Tufts Medical Center
MedicalResearch.com: What is the background for this study?
Response: Hypertension affects nearly half of all adults in the United States and is a major risk factor for many serious health conditions. Fortunately, by screening all adults for hypertension, clinicians can improve their patient’s health. The Task Force continues to recommend screening all adults for hypertension so that they can get the care they need to help prevent health conditions such as heart attack, stroke, and kidney failure.
Dr. Wong[/caption]
John B. Wong, M.D.
Chief Scientific Officer
Vice chair for Clinical Affairs
Chief of the Division of Clinical Decision Making and
Primary care Clinician
Department of Medicine at Tufts Medical Center
MedicalResearch.com: What is the background for this study?
Response: Hypertension affects nearly half of all adults in the United States and is a major risk factor for many serious health conditions. Fortunately, by screening all adults for hypertension, clinicians can improve their patient’s health. The Task Force continues to recommend screening all adults for hypertension so that they can get the care they need to help prevent health conditions such as heart attack, stroke, and kidney failure.

 As a specialized healthcare position where you will be responsible for the health and wellbeing of patients, nurses are required to hold a degree and a license before they can begin work. To qualify as a registered nurse, you will need to obtain a BSN degree, which typically takes around four years when studying full-time. However, if you already have a bachelor’s degree in another subject, there is an option that will allow you to become a nurse in half the time; accelerated nursing programs are designed for those who already have a bachelor’s degree and want a quick career change into nursing. The
As a specialized healthcare position where you will be responsible for the health and wellbeing of patients, nurses are required to hold a degree and a license before they can begin work. To qualify as a registered nurse, you will need to obtain a BSN degree, which typically takes around four years when studying full-time. However, if you already have a bachelor’s degree in another subject, there is an option that will allow you to become a nurse in half the time; accelerated nursing programs are designed for those who already have a bachelor’s degree and want a quick career change into nursing. The 

 Dr. Bunik[/caption]
Maya Bunik, MD, MPH | Professor, Pediatrics
Medical Director, Child Health Clinic, Primary Care | Breastfeeding Management Clinic
Adult and Child Consortium for Health Outcomes Research and Delivery Science (ACCORDS)
School of Medicine| University of Colorado Anschutz Medical Campus
Children's Hospital Colorado
MedicalResearch.com: What is the background for this study?
Response: Marijuana legalization has been increasing in the United States, with increasing consumption of marijuana products. Currently, the American Academy of Pediatrics (AAP), American College of Obstetricians and Gynecologists (ACOG) and Academy of Breastfeeding Medicine (ABM) do not recommend marijuana use during pregnancy or lactation due to concerning though limited data on the effects of perinatal marijuana exposure.
As there has been increasing prevalence of women using marijuana during pregnancy due to legalization and perceptions of safety, we sought to determine the duration of THC excretion in breast milk among women who had evidence of marijuana use at delivery and abstained post-partum.
Dr. Bunik[/caption]
Maya Bunik, MD, MPH | Professor, Pediatrics
Medical Director, Child Health Clinic, Primary Care | Breastfeeding Management Clinic
Adult and Child Consortium for Health Outcomes Research and Delivery Science (ACCORDS)
School of Medicine| University of Colorado Anschutz Medical Campus
Children's Hospital Colorado
MedicalResearch.com: What is the background for this study?
Response: Marijuana legalization has been increasing in the United States, with increasing consumption of marijuana products. Currently, the American Academy of Pediatrics (AAP), American College of Obstetricians and Gynecologists (ACOG) and Academy of Breastfeeding Medicine (ABM) do not recommend marijuana use during pregnancy or lactation due to concerning though limited data on the effects of perinatal marijuana exposure.
As there has been increasing prevalence of women using marijuana during pregnancy due to legalization and perceptions of safety, we sought to determine the duration of THC excretion in breast milk among women who had evidence of marijuana use at delivery and abstained post-partum. 
 Dr. Pollard[/caption]
Michael S. Pollard, Ph.D.
Professor, Pardee RAND Graduate School
Senior Sociologist
RAND Corporation
Santa Monica, CA 90407-2138
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: There are ample anecdotal jokes and stories about increased alcohol use during COVID-19 and stay-at-home orders. Our study provides robust longitudinal evidence that people drank more frequently, and for women in particular, more heavily, and with more negative consequences, during the initial stages of COVID-19 compared to their own behaviors from a year earlier (May/June 2020 compared to May/June 2019). Women’s alcohol consumption was most significantly changed, with a 17% increase in number of days drinking, and a 41% increase in days of binge drinking (when they had four or more drinks in a couple of hours). This means that, nationally, one in five women drank heavily one more day a month than the same time in 2019, on average. Women also reported a 39% increase in alcohol-related problems, such as “I took foolish risks” or “I failed to do what was expected of me” because of drinking alcohol.
Dr. Pollard[/caption]
Michael S. Pollard, Ph.D.
Professor, Pardee RAND Graduate School
Senior Sociologist
RAND Corporation
Santa Monica, CA 90407-2138
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: There are ample anecdotal jokes and stories about increased alcohol use during COVID-19 and stay-at-home orders. Our study provides robust longitudinal evidence that people drank more frequently, and for women in particular, more heavily, and with more negative consequences, during the initial stages of COVID-19 compared to their own behaviors from a year earlier (May/June 2020 compared to May/June 2019). Women’s alcohol consumption was most significantly changed, with a 17% increase in number of days drinking, and a 41% increase in days of binge drinking (when they had four or more drinks in a couple of hours). This means that, nationally, one in five women drank heavily one more day a month than the same time in 2019, on average. Women also reported a 39% increase in alcohol-related problems, such as “I took foolish risks” or “I failed to do what was expected of me” because of drinking alcohol.








