

 Source[/caption]
Taking the first step towards better hearing can be both exciting and a little intimidating. Whether you’ve noticed a gradual change in your hearing or a loved one has suggested it might be time for a check-up, scheduling that first appointment is an important move toward improving your overall quality of life. For those considering professional hearing care in Kitchener, understanding what to expect during your initial visit can make the process much smoother and help you feel more prepared.
This guide walks you through each stage of your first appointment— from the moment you walk in the door to your post-visit plan. If you’ve never been to a hearing clinic before, you’ll discover that modern hearing care is both comprehensive and highly personalized.
Source[/caption]
Taking the first step towards better hearing can be both exciting and a little intimidating. Whether you’ve noticed a gradual change in your hearing or a loved one has suggested it might be time for a check-up, scheduling that first appointment is an important move toward improving your overall quality of life. For those considering professional hearing care in Kitchener, understanding what to expect during your initial visit can make the process much smoother and help you feel more prepared.
This guide walks you through each stage of your first appointment— from the moment you walk in the door to your post-visit plan. If you’ve never been to a hearing clinic before, you’ll discover that modern hearing care is both comprehensive and highly personalized.
 Living with tinnitus often feels like a constant battle against sounds that refuse to fade. Whether it’s a high-pitched ringing, a steady hum, or an unpredictable buzzing, the condition can disrupt nearly every part of daily life. Sleep becomes difficult, focus weakens, and the emotional toll can be overwhelming. For years, available treatments have focused more on managing symptoms than providing lasting relief.
Now, that’s beginning to change. Advances in neuroscience, medical research, and technology are uncovering the underlying causes of tinnitus, bringing a wave of new treatments that go beyond simply masking the noise. The potential for lasting relief—or even complete elimination—feels closer than ever.
One particularly exciting development is paired stimulation, which integrates sound therapy with electrical or magnetic pulses. This approach to tinnitus patients is designed to retrain the brain’s response to tinnitus by strengthening normal auditory pathways while weakening abnormal ones. Early studies suggest that regular sessions may lead to long-term improvements, even after treatment ends. Clinics like Regain Hearing are closely monitoring these advancements, ensuring that individuals with tinnitus have access to the latest diagnostic tools and therapies as they become available.
While neuromodulation remains in the experimental stage, ongoing clinical trials continue to refine these techniques. Personalized therapies tailored to an individual’s specific tinnitus profile may soon become widely accessible, offering new options for those who have struggled to find effective solutions.
Living with tinnitus often feels like a constant battle against sounds that refuse to fade. Whether it’s a high-pitched ringing, a steady hum, or an unpredictable buzzing, the condition can disrupt nearly every part of daily life. Sleep becomes difficult, focus weakens, and the emotional toll can be overwhelming. For years, available treatments have focused more on managing symptoms than providing lasting relief.
Now, that’s beginning to change. Advances in neuroscience, medical research, and technology are uncovering the underlying causes of tinnitus, bringing a wave of new treatments that go beyond simply masking the noise. The potential for lasting relief—or even complete elimination—feels closer than ever.
One particularly exciting development is paired stimulation, which integrates sound therapy with electrical or magnetic pulses. This approach to tinnitus patients is designed to retrain the brain’s response to tinnitus by strengthening normal auditory pathways while weakening abnormal ones. Early studies suggest that regular sessions may lead to long-term improvements, even after treatment ends. Clinics like Regain Hearing are closely monitoring these advancements, ensuring that individuals with tinnitus have access to the latest diagnostic tools and therapies as they become available.
While neuromodulation remains in the experimental stage, ongoing clinical trials continue to refine these techniques. Personalized therapies tailored to an individual’s specific tinnitus profile may soon become widely accessible, offering new options for those who have struggled to find effective solutions.
 Photo by Photo By: Kaboompics.com[/caption]
Photo by Photo By: Kaboompics.com[/caption]


One step at a time, hearing aids are becoming an almost mandatory part of the superior hearing experience....
 Dr. Reed[/caption]
Nicholas S. Reed, AuD PhD
Assistant Professor | Department of Epidemiology
Johns Hopkins University Bloomberg School of Public Health
MedicalResearch.com: What is the background for this study?
Response: To date, national estimates of hearing loss have often been based on self-report, which is a fine metric in its own right but underestimates the prevalence of hearing loss against criterion standard measures, and most studies with criterion-level hearing measures are limited to relatively younger samples of older adults. For example, some previous nationally representative samples don't allow reporting age data over 80 years because there aren't enough participants in that age group. It is not surprising given that it is difficult to design nationally representative studies that truly allow older adults (80+ years) to participate and measuring hearing can be onerous. However, understanding the prevalence of hearing loss in this age group is vital for public health and policy planning efforts to address hearing loss at the national level.
Dr. Reed[/caption]
Nicholas S. Reed, AuD PhD
Assistant Professor | Department of Epidemiology
Johns Hopkins University Bloomberg School of Public Health
MedicalResearch.com: What is the background for this study?
Response: To date, national estimates of hearing loss have often been based on self-report, which is a fine metric in its own right but underestimates the prevalence of hearing loss against criterion standard measures, and most studies with criterion-level hearing measures are limited to relatively younger samples of older adults. For example, some previous nationally representative samples don't allow reporting age data over 80 years because there aren't enough participants in that age group. It is not surprising given that it is difficult to design nationally representative studies that truly allow older adults (80+ years) to participate and measuring hearing can be onerous. However, understanding the prevalence of hearing loss in this age group is vital for public health and policy planning efforts to address hearing loss at the national level.

 Dr. Reed[/caption]
Nicholas S. Reed, AuD
Assistant Professor | Department of Epidemiology
Core Faculty | Cochlear Center for Hearing and Public Health
Johns Hopkins University Bloomberg School of Public Health
MedicalResearch.com: What is the background for this study?
Response: It is known that hearing aid ownership is relatively low in the United States at less than 20% of adults with hearing loss owning and using hearing aids. However, many national estimates of hearing aid ownership are based on data that is over 10 years old. Our team was interested in trying to understand whether ownership in hearing aids had changed over time. We used data from 2011 to 2018 in a nationally representative (United States) observational cohort (The National Health and Aging Trends Study) of Medicare Beneficiaries aged 70 years and older to estimate the change in hearing aid ownership.
In our analysis, the proportion of Medicare beneficiaries 70 years and older who reported owning and using their hearing aids increased 23.3% from 2011 to 2018. However, this growth in ownership was not equal across all older adults. For example, while White males saw a 28.7% increase in hearing aid ownership, Black females saw only a 5.8% increase over the same 8-year period. Moreover, adults living at less than 100% federal poverty level actually saw an overall 13.0% decrease in hearing aid ownership while those living at more than 200% federal poverty line saw an overall 30.6% increase.
Dr. Reed[/caption]
Nicholas S. Reed, AuD
Assistant Professor | Department of Epidemiology
Core Faculty | Cochlear Center for Hearing and Public Health
Johns Hopkins University Bloomberg School of Public Health
MedicalResearch.com: What is the background for this study?
Response: It is known that hearing aid ownership is relatively low in the United States at less than 20% of adults with hearing loss owning and using hearing aids. However, many national estimates of hearing aid ownership are based on data that is over 10 years old. Our team was interested in trying to understand whether ownership in hearing aids had changed over time. We used data from 2011 to 2018 in a nationally representative (United States) observational cohort (The National Health and Aging Trends Study) of Medicare Beneficiaries aged 70 years and older to estimate the change in hearing aid ownership.
In our analysis, the proportion of Medicare beneficiaries 70 years and older who reported owning and using their hearing aids increased 23.3% from 2011 to 2018. However, this growth in ownership was not equal across all older adults. For example, while White males saw a 28.7% increase in hearing aid ownership, Black females saw only a 5.8% increase over the same 8-year period. Moreover, adults living at less than 100% federal poverty level actually saw an overall 13.0% decrease in hearing aid ownership while those living at more than 200% federal poverty line saw an overall 30.6% increase.


 Dr. Wick[/caption]
Cameron C. Wick, MD
Assistant Professor, Otology/Neurotology
Washington University School of Medicine
St. Louis, MO
MedicalResearch.com: What do you see as the primary message of your findings for the general public?
Response: Older adults not satisfied with their hearing aids achieved clinically meaningful improvement in both hearing and quality of life with a cochlear implant compared to an optimized bilateral hearing aid condition.
MedicalResearch.com: Do you see your findings as changing the way older adults with hearing loss are managed?
Response: Yes and partially because this study is unique in its design and the outcomes that were measured. Specifically the study is a prospective, multicenter clinical trial conducted at 13 locations across the United States. All patients were setup with a 30-day optimized hearing aid experience before cochlear implantation (context: sometimes hearing aids are not appropriately optimized so baseline testing may not reflect the "best" that hearing aids can do). This study assesses both hearing data as well as quality of life data before and 6-months after cochlear implantation. After implantation patients were tested in both the unilateral (cochlear implant alone) and bimodal (cochlear implant plus hearing aid in the opposite ear) conditions. My paper is a subanalysis of adults 65 years and older (range 65 - 91 years) enrolled in the clinical trial. The principal investigator of the clinical trial is Dr. Craig Buchman. Dr. Buchman and myself are at Washington University in St. Louis which was the lead center for the clinical trial.
The findings of the study are meaningful because they demonstrate clear superiority of cochlear implants over hearing aids in many key areas, such as understanding speech, hearing in background noise, and ability to communicate. Hearing loss, which becomes more prevalent as we age, can negatively impact communication leading to social isolation, depression, frustration, and possibly cognitive decline. This study highlights that if patients are not satisfied with their hearing aid performance then they should be referred to a center that can evaluate for cochlear implantation. Cochlear implant indications have evolved considerably since they were first FDA approved in 1984. This study emphasizes that patients do not have to be profoundly deaf to experience significant hearing and social benefits from cochlear implants. Also, it demonstrates that cochlear implant surgery is well tolerated even as adults age and acquire other health ailments.
Dr. Wick[/caption]
Cameron C. Wick, MD
Assistant Professor, Otology/Neurotology
Washington University School of Medicine
St. Louis, MO
MedicalResearch.com: What do you see as the primary message of your findings for the general public?
Response: Older adults not satisfied with their hearing aids achieved clinically meaningful improvement in both hearing and quality of life with a cochlear implant compared to an optimized bilateral hearing aid condition.
MedicalResearch.com: Do you see your findings as changing the way older adults with hearing loss are managed?
Response: Yes and partially because this study is unique in its design and the outcomes that were measured. Specifically the study is a prospective, multicenter clinical trial conducted at 13 locations across the United States. All patients were setup with a 30-day optimized hearing aid experience before cochlear implantation (context: sometimes hearing aids are not appropriately optimized so baseline testing may not reflect the "best" that hearing aids can do). This study assesses both hearing data as well as quality of life data before and 6-months after cochlear implantation. After implantation patients were tested in both the unilateral (cochlear implant alone) and bimodal (cochlear implant plus hearing aid in the opposite ear) conditions. My paper is a subanalysis of adults 65 years and older (range 65 - 91 years) enrolled in the clinical trial. The principal investigator of the clinical trial is Dr. Craig Buchman. Dr. Buchman and myself are at Washington University in St. Louis which was the lead center for the clinical trial.
The findings of the study are meaningful because they demonstrate clear superiority of cochlear implants over hearing aids in many key areas, such as understanding speech, hearing in background noise, and ability to communicate. Hearing loss, which becomes more prevalent as we age, can negatively impact communication leading to social isolation, depression, frustration, and possibly cognitive decline. This study highlights that if patients are not satisfied with their hearing aid performance then they should be referred to a center that can evaluate for cochlear implantation. Cochlear implant indications have evolved considerably since they were first FDA approved in 1984. This study emphasizes that patients do not have to be profoundly deaf to experience significant hearing and social benefits from cochlear implants. Also, it demonstrates that cochlear implant surgery is well tolerated even as adults age and acquire other health ailments.

 Dr. Blundon[/caption]
Elizabeth Blundon PhD
Department of Psychology
University of British Columbia – Vancouver
MedicalResearch.com: What is the background for this study?
Response: Many healthcare workers have noticed that dying patients appear to be comforted by the words of their loved ones, even when patients appear to be unconscious and are no longer able to communicate. There is a persistent belief, therefore, that hearing may persist into the last hours of someone's life. Our study attempts to detect evidence of hearing among a small group of unresponsive hospice patients at the end of life.
To do this, we compared the brain activity of young, healthy control participants, with the brain activity of hospice patients, both when the patients were awake and responsive, and again when they became unresponsive. The brain activity we measured was in response to a complex series of tone-patterns, where participants were asked to identify by pressing a button (control participants) or by counting (hospice patients) every time they heard a tone-pattern that was different from the rest of the series.
Dr. Blundon[/caption]
Elizabeth Blundon PhD
Department of Psychology
University of British Columbia – Vancouver
MedicalResearch.com: What is the background for this study?
Response: Many healthcare workers have noticed that dying patients appear to be comforted by the words of their loved ones, even when patients appear to be unconscious and are no longer able to communicate. There is a persistent belief, therefore, that hearing may persist into the last hours of someone's life. Our study attempts to detect evidence of hearing among a small group of unresponsive hospice patients at the end of life.
To do this, we compared the brain activity of young, healthy control participants, with the brain activity of hospice patients, both when the patients were awake and responsive, and again when they became unresponsive. The brain activity we measured was in response to a complex series of tone-patterns, where participants were asked to identify by pressing a button (control participants) or by counting (hospice patients) every time they heard a tone-pattern that was different from the rest of the series.

 Dr. Sarant[/caption]
Julia Sarant, PhD
Associate Professor
Department of Audiology and Speech Pathology
Faculty of Medicine, Dentistry and Health Sciences
Melbourne School of Health Sciences
MedicalResearch.com: What is the background for this study?
Response: Dementia is a rapidly growing global problem. Hearing loss has been identified by the Lancet Commissions as a modifiable risk factor for dementia. There is no treatment for dementia.
This study investigated the effect of hearing aid use on cognition over time in older adults, objectively assessing hearing loss treatment, compliance and benefits while controlling for the effects of other known risk factors for dementia.
Dr. Sarant[/caption]
Julia Sarant, PhD
Associate Professor
Department of Audiology and Speech Pathology
Faculty of Medicine, Dentistry and Health Sciences
Melbourne School of Health Sciences
MedicalResearch.com: What is the background for this study?
Response: Dementia is a rapidly growing global problem. Hearing loss has been identified by the Lancet Commissions as a modifiable risk factor for dementia. There is no treatment for dementia.
This study investigated the effect of hearing aid use on cognition over time in older adults, objectively assessing hearing loss treatment, compliance and benefits while controlling for the effects of other known risk factors for dementia.
 Dr. Parthasarathy[/caption]
Aravindakshan Parthasarathy, PhD
Researcher, Massachusetts Eye and Ear
Instructor in Otolaryngology–Head and Neck Surgery
Harvard Medical School
MedicalResearch.com: What is the background for this study? Would you briefly explain what is meant by Hidden Hearing Loss?
Response: Our ears were not designed for the society our brains created. The World Health Organization estimates that 1 billion young adults are at risk for hearing loss due to prolonged exposure to excessive environmental noise. Anatomical analysis of human ears has shown that half of the nerve fibers connecting the ear to the brain have degenerated by the time we reach 40 years of age. Many of us experience the first symptoms of hearing loss as a difficulty following conversations in crowded places such as restaurants.
Hidden hearing loss is an umbrella term used to describe such hearing difficulties experienced by people who show no abnormalities on any of the current tests of hearing used in the clinic. Approximately 10% of visitors to our hospital hearing clinic fit this profile, arriving with a primary complaint of poor hearing but being sent home with a clean bill of hearing health.
Dr. Parthasarathy[/caption]
Aravindakshan Parthasarathy, PhD
Researcher, Massachusetts Eye and Ear
Instructor in Otolaryngology–Head and Neck Surgery
Harvard Medical School
MedicalResearch.com: What is the background for this study? Would you briefly explain what is meant by Hidden Hearing Loss?
Response: Our ears were not designed for the society our brains created. The World Health Organization estimates that 1 billion young adults are at risk for hearing loss due to prolonged exposure to excessive environmental noise. Anatomical analysis of human ears has shown that half of the nerve fibers connecting the ear to the brain have degenerated by the time we reach 40 years of age. Many of us experience the first symptoms of hearing loss as a difficulty following conversations in crowded places such as restaurants.
Hidden hearing loss is an umbrella term used to describe such hearing difficulties experienced by people who show no abnormalities on any of the current tests of hearing used in the clinic. Approximately 10% of visitors to our hospital hearing clinic fit this profile, arriving with a primary complaint of poor hearing but being sent home with a clean bill of hearing health.

 Dr. Blustein[/caption]
Jan Blustein, MD PhD
Professor of Health Policy and Medicine
Wagner Graduate School and School of Medicine
New York University, New York
MedicalResearch.com: What is the background for this study?
Response: The National Institutes of Health (NIH), the nation’s largest public funder of health research, provides annual reports about levels of funding for many diseases and conditions. These reports, issued as part of the NIH’s Research, Condition and Disease Categorization (RCDC) process, allow members of the public to track funding across key conditions and across time.
Hearing loss is not included among the reported conditions. This runs counter to two of the NIH’s stated goals, according to researcher Jan Blustein (M.D., Ph.D.), professor of health policy and medicine at New York University’s Robert F. Wagner Graduate School of Public Service, in a Research Letter in the May 15th issue of the Journal of the American Medical Association Otolaryngology and Head & Neck Surgery.
“First, the NIH is committed to transparency about how it divides funds across diseases and conditions,” said Dr. Blustein. “Second, it has said that it will prioritize its funding to those conditions that cause the greatest disease burden.” Hearing loss causes great disease burden, ranking 10th in the U.S. among all conditions as a contributor to Disability Adjusted Life Years (a widely-used measure of disease burden), according to the World Health Organization.
Dr. Blustein[/caption]
Jan Blustein, MD PhD
Professor of Health Policy and Medicine
Wagner Graduate School and School of Medicine
New York University, New York
MedicalResearch.com: What is the background for this study?
Response: The National Institutes of Health (NIH), the nation’s largest public funder of health research, provides annual reports about levels of funding for many diseases and conditions. These reports, issued as part of the NIH’s Research, Condition and Disease Categorization (RCDC) process, allow members of the public to track funding across key conditions and across time.
Hearing loss is not included among the reported conditions. This runs counter to two of the NIH’s stated goals, according to researcher Jan Blustein (M.D., Ph.D.), professor of health policy and medicine at New York University’s Robert F. Wagner Graduate School of Public Service, in a Research Letter in the May 15th issue of the Journal of the American Medical Association Otolaryngology and Head & Neck Surgery.
“First, the NIH is committed to transparency about how it divides funds across diseases and conditions,” said Dr. Blustein. “Second, it has said that it will prioritize its funding to those conditions that cause the greatest disease burden.” Hearing loss causes great disease burden, ranking 10th in the U.S. among all conditions as a contributor to Disability Adjusted Life Years (a widely-used measure of disease burden), according to the World Health Organization.
 Dr. Schneider[/caption]
Keith Schneider PhD
Director, Center for Biomedical and Brain Imaging
Associate Professor
Department of Psychological and Brain Sciences
University of Delaware
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Absolute pitch is the ability to name a musical note in isolation. It is rare in the population, approximately 1/10,000 people have it. The neural mechanisms of this ability have not been clear. It is not known whether people with absolute pitch encode auditory frequencies differently, or whether absolute pitch derives from the same sensory encoding but different memory connections.
We tested 20 people with absolute pitch, 20 matched musicians with the same number of years of musical training, age of onset of musical training, and number of hours of practice per week, as well as 20 controls with minimal musical training.
The main findings are that people with absolute pitch have larger early auditory cortex—primary auditory cortex was enlarged about 50% relative to the other two groups, which did not differ significantly from each other. We also found that the tuning bandwidth of the individual voxels in the early auditory cortical areas was broader in people with absolute pitch.
That is, these small bits of the brain responded to a wide range of frequencies than those in the other two groups. This suggested to us that people with absolute pitch might imply what is known as “ensemble encoding”. That is, they use a larger network of neurons to encode sounds.
Dr. Schneider[/caption]
Keith Schneider PhD
Director, Center for Biomedical and Brain Imaging
Associate Professor
Department of Psychological and Brain Sciences
University of Delaware
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Absolute pitch is the ability to name a musical note in isolation. It is rare in the population, approximately 1/10,000 people have it. The neural mechanisms of this ability have not been clear. It is not known whether people with absolute pitch encode auditory frequencies differently, or whether absolute pitch derives from the same sensory encoding but different memory connections.
We tested 20 people with absolute pitch, 20 matched musicians with the same number of years of musical training, age of onset of musical training, and number of hours of practice per week, as well as 20 controls with minimal musical training.
The main findings are that people with absolute pitch have larger early auditory cortex—primary auditory cortex was enlarged about 50% relative to the other two groups, which did not differ significantly from each other. We also found that the tuning bandwidth of the individual voxels in the early auditory cortical areas was broader in people with absolute pitch.
That is, these small bits of the brain responded to a wide range of frequencies than those in the other two groups. This suggested to us that people with absolute pitch might imply what is known as “ensemble encoding”. That is, they use a larger network of neurons to encode sounds.
 Dr. Cederroth[/caption]
Christopher R. Cederroth | Ph.D. Docent
Associate Professor
Experimental Audiology | Department of Physiology and Pharmacology
Karolinska Institutet
Sweden
MedicalResearch.com: What is the background for this study?
Response: Tinnitus is experienced is experienced by a large proportion of the population and affects more than 15% of the population worldwide (estimated 70 million people in Europe). However, for near 3% of the population, tinnitus becomes a chronic bothersome and incapacitating symptom. Severe tinnitus interferes with sleep, mood, and concentration and thus impacts life quality, ultimately leading to sick leave and disability pension. A high cost to society has been reported, and since the prevalence of tinnitus has been predicted to double in Europe by 2050, there is an important need for an effective treatment. And today there are none, with the exception of cognitive behavioral therapy, which helps coping with it but does not remove the tinnitus. There has been a number of innovative treatment approaches, but they are overall not successful and it is now agreed that it is likely because tinnitus is a heterogeneous condition – meaning that we cannot consider tinnitus a single entity but an ensemble of different forms or subtypes, which need to be defined.
Tinnitus has always been considered a condition influenced by environmental factors, but our initial studies suggested the opposite. Adoption studies are excellent in showing the influence of shared-environment effects and establish a genetic basis for a disease or a trait. It allows to test the transmission of a trait between the adoptee and their biological or their adoptive parent. Transmission via the biological parent is expected to be due to a heritable genetic effect, while transmission via the adoptive parent is associated with home-environment, the so-called shared-environmental effect. We used medical registry data to identify tinnitus patients and adoptees.
Dr. Cederroth[/caption]
Christopher R. Cederroth | Ph.D. Docent
Associate Professor
Experimental Audiology | Department of Physiology and Pharmacology
Karolinska Institutet
Sweden
MedicalResearch.com: What is the background for this study?
Response: Tinnitus is experienced is experienced by a large proportion of the population and affects more than 15% of the population worldwide (estimated 70 million people in Europe). However, for near 3% of the population, tinnitus becomes a chronic bothersome and incapacitating symptom. Severe tinnitus interferes with sleep, mood, and concentration and thus impacts life quality, ultimately leading to sick leave and disability pension. A high cost to society has been reported, and since the prevalence of tinnitus has been predicted to double in Europe by 2050, there is an important need for an effective treatment. And today there are none, with the exception of cognitive behavioral therapy, which helps coping with it but does not remove the tinnitus. There has been a number of innovative treatment approaches, but they are overall not successful and it is now agreed that it is likely because tinnitus is a heterogeneous condition – meaning that we cannot consider tinnitus a single entity but an ensemble of different forms or subtypes, which need to be defined.
Tinnitus has always been considered a condition influenced by environmental factors, but our initial studies suggested the opposite. Adoption studies are excellent in showing the influence of shared-environment effects and establish a genetic basis for a disease or a trait. It allows to test the transmission of a trait between the adoptee and their biological or their adoptive parent. Transmission via the biological parent is expected to be due to a heritable genetic effect, while transmission via the adoptive parent is associated with home-environment, the so-called shared-environmental effect. We used medical registry data to identify tinnitus patients and adoptees.

 MedicalResearch.com Interview with:
Dr. Véronique J. C. Kraaijenga MD
Department of Otorhinolaryngology–Head and Neck Surgery
Brain Center Rudolf Magnus, University Medical Center Utrecht, Utrecht, the Netherlands
MedicalResearch.com: What is the background for this study?
Response: During the past two decades, the frequency of hearing loss among young people has increased and going to music concerts, clubs and festivals may part of the reason. Noise-induced hearing loss because of recreational noise exposure is reduced by using earplugs.
Our study evaluated 51 adults who attended an outdoor music festival in Amsterdam, the Netherlands, in September 2015. The study measured music festival visit for 4.5 hours (intervention); temporary hearing loss (outcome).
MedicalResearch.com Interview with:
Dr. Véronique J. C. Kraaijenga MD
Department of Otorhinolaryngology–Head and Neck Surgery
Brain Center Rudolf Magnus, University Medical Center Utrecht, Utrecht, the Netherlands
MedicalResearch.com: What is the background for this study?
Response: During the past two decades, the frequency of hearing loss among young people has increased and going to music concerts, clubs and festivals may part of the reason. Noise-induced hearing loss because of recreational noise exposure is reduced by using earplugs.
Our study evaluated 51 adults who attended an outdoor music festival in Amsterdam, the Netherlands, in September 2015. The study measured music festival visit for 4.5 hours (intervention); temporary hearing loss (outcome).
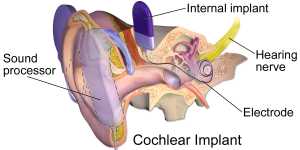 An illustration of a cochlear implant: Wikipedia image[/caption]
Niki Katerina Vavatzanidis MSc
Department of Neuropsychology
Max Planck Institute for Human and Cognitive Brain Science
Leipzig, Germany
Technische Universität Dresden, Germany
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Cochlear implants (CIs) are a way of providing hearing to sensorineural deaf individuals. The implant works by first picking up sounds from the environment and transforming them into an electric signal. Via an array of electrodes the implant then transmits the signal directly to the auditory nerve, which then leads to auditory sensations in the brain.
In our study, we were interested to see how language acquisition is affected when language immersion occurs at an untypically late age. Children with cochlear implants that grow up in exclusively or predominantly hearing environments will have their first language encounter at the time of implantation, which nowadays is roughly between the age of one and three. Besides the later starting point in language acquisition, children with CIs are facing a compromised input quality compared to typical hearing.
We know from typically hearing children that it is around the age of 14 months that their vocabulary becomes robust enough to react to name violations. That is, when a picture is labelled incorrectly, their brain waves will display with the so-called N400 effect. In our study we were interested whether children with CIs would also show the N400 effect and if so, how many months of hearing experience are necessary. We measured the brain activity of children implanted between the age of one and four at three time points: 12, 18, and 24 months after implant activation. To our surprise, congenitally deaf children whose only language input had been via the cochlear implant already displayed the N400 effect after 12 months of language immersion, i.e. earlier than seen in typically hearing children.
An illustration of a cochlear implant: Wikipedia image[/caption]
Niki Katerina Vavatzanidis MSc
Department of Neuropsychology
Max Planck Institute for Human and Cognitive Brain Science
Leipzig, Germany
Technische Universität Dresden, Germany
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Cochlear implants (CIs) are a way of providing hearing to sensorineural deaf individuals. The implant works by first picking up sounds from the environment and transforming them into an electric signal. Via an array of electrodes the implant then transmits the signal directly to the auditory nerve, which then leads to auditory sensations in the brain.
In our study, we were interested to see how language acquisition is affected when language immersion occurs at an untypically late age. Children with cochlear implants that grow up in exclusively or predominantly hearing environments will have their first language encounter at the time of implantation, which nowadays is roughly between the age of one and three. Besides the later starting point in language acquisition, children with CIs are facing a compromised input quality compared to typical hearing.
We know from typically hearing children that it is around the age of 14 months that their vocabulary becomes robust enough to react to name violations. That is, when a picture is labelled incorrectly, their brain waves will display with the so-called N400 effect. In our study we were interested whether children with CIs would also show the N400 effect and if so, how many months of hearing experience are necessary. We measured the brain activity of children implanted between the age of one and four at three time points: 12, 18, and 24 months after implant activation. To our surprise, congenitally deaf children whose only language input had been via the cochlear implant already displayed the N400 effect after 12 months of language immersion, i.e. earlier than seen in typically hearing children.
 David G. Loughrey, BA(Hons)
NEIL (Neuro Enhancement for Independent Lives) Programme
Trinity College Institute of Neuroscience, School of Medicine
Trinity College Dublin, Dublin, Ireland
MedicalResearch.com: What is the background for this study?
Response: Age-related hearing loss, a common chronic condition among older adults, has emerged in the literature as a potential modifiable risk factor for dementia. This is of interest as current pharmacological therapies for dementias such as Alzheimer’s disease only offer symptom-modifying effects. Treatment of risk factors such as hearing loss may help delay the onset of dementia and may provide an alternate therapeutic strategy. However, there is variance in the research on hearing loss and cognition with some studies reporting a small or non-significant association. In this meta-analysis, we investigated this association and we only included observational studies that used standard assessments of cognitive function and pure-tone audiometry (the clinical standard).
David G. Loughrey, BA(Hons)
NEIL (Neuro Enhancement for Independent Lives) Programme
Trinity College Institute of Neuroscience, School of Medicine
Trinity College Dublin, Dublin, Ireland
MedicalResearch.com: What is the background for this study?
Response: Age-related hearing loss, a common chronic condition among older adults, has emerged in the literature as a potential modifiable risk factor for dementia. This is of interest as current pharmacological therapies for dementias such as Alzheimer’s disease only offer symptom-modifying effects. Treatment of risk factors such as hearing loss may help delay the onset of dementia and may provide an alternate therapeutic strategy. However, there is variance in the research on hearing loss and cognition with some studies reporting a small or non-significant association. In this meta-analysis, we investigated this association and we only included observational studies that used standard assessments of cognitive function and pure-tone audiometry (the clinical standard).
 Dr. Carlijn M. P. le Clercq[/caption]
Dr. Carlijn M. P. le Clercq, MD
Speech and Language Pathology, Pediatrics, Otolaryngology
Erasmus MC , Rotterdam
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: There has been increasing interest for acquired hearing loss among children, and concerns about its prevalence possibly rising over time. One of the questions that come up, is whether there is an association with the growing use of portable music players with headphones, including smartphones and tablets. There have been few longitudinal studies to explore this relation.
In order to examine this relation, among other factors, we have conducted a formal hearing screening among more than 5000 9- to 11-year-old children from a population-based birth cohort in the Netherlands.
Our study showed that nearly one in five children did not have normal hearing. Of the cohort, 7.8% of the children showed signs of permanent hearing loss.
Dr. Carlijn M. P. le Clercq[/caption]
Dr. Carlijn M. P. le Clercq, MD
Speech and Language Pathology, Pediatrics, Otolaryngology
Erasmus MC , Rotterdam
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: There has been increasing interest for acquired hearing loss among children, and concerns about its prevalence possibly rising over time. One of the questions that come up, is whether there is an association with the growing use of portable music players with headphones, including smartphones and tablets. There have been few longitudinal studies to explore this relation.
In order to examine this relation, among other factors, we have conducted a formal hearing screening among more than 5000 9- to 11-year-old children from a population-based birth cohort in the Netherlands.
Our study showed that nearly one in five children did not have normal hearing. Of the cohort, 7.8% of the children showed signs of permanent hearing loss.
 Jan Janssen, Senior Vice President
Research and Development
Cochlear Limited
MedicalResearch.com: What is the background for this device?
Response: Cochlear implants treat hearing loss by electrical stimulation of the hearing nerve, bypassing the damaged parts of the hearing pathway. Cochlear implants system consist out of an external sound processor that detects and processes the sounds and then sends them to the implant. The implant receives this information and turns it into electrical signals that are delivered to the hearing nerve and from there to the brain.
The Nucleus® 7 Sound Processor is the world’s first and only Made for iPhone cochlear implant sound processor, allowing users to stream sound from their iPhone®, iPad® and iPod touch® directly to their cochlear implant sound processor. It not only enhances the experience of talking on the phone, it also makes features like enjoying music or watching videos, as well as audio apps such as Maps or FaceTime, more easily accessible.
The Nucleus 7 Sound Processor is also the smallest and lightest behind-the-ear sound processor on the market.
Jan Janssen, Senior Vice President
Research and Development
Cochlear Limited
MedicalResearch.com: What is the background for this device?
Response: Cochlear implants treat hearing loss by electrical stimulation of the hearing nerve, bypassing the damaged parts of the hearing pathway. Cochlear implants system consist out of an external sound processor that detects and processes the sounds and then sends them to the implant. The implant receives this information and turns it into electrical signals that are delivered to the hearing nerve and from there to the brain.
The Nucleus® 7 Sound Processor is the world’s first and only Made for iPhone cochlear implant sound processor, allowing users to stream sound from their iPhone®, iPad® and iPod touch® directly to their cochlear implant sound processor. It not only enhances the experience of talking on the phone, it also makes features like enjoying music or watching videos, as well as audio apps such as Maps or FaceTime, more easily accessible.
The Nucleus 7 Sound Processor is also the smallest and lightest behind-the-ear sound processor on the market.
 Dr. Nicholas Reed[/caption]
Nicholas S. Reed, AuD
Instructor | Department of Otolaryngology-Head/Neck Surgery
PhD Candidate | Graduate Training Program in Clinical Investigation
Center on Aging and Health
Johns Hopkins University School of Medicine
Johns Hopkins University Bloomberg School of Public Health
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Hearing Aids are medical devices regulated by the FDA which must be purchased through a licensed individual while personal sound amplification products (PSAPs) are essentially unregulated devices some of which can manipulate and increase sound similar to a hearing aid but cannot market themselves are devices for hearing loss. PSAPs can be purchased online or in the back of a store and are generally less expensive than hearing aids.
We aimed to explore a select group of PSAPs to see if they helped someone with mild to moderate hearing loss improve speech understanding (i.e. ability to repeat back sentences) in the presence of mild background noise (think a lunch crowd at a restaurant) as well as a hearing aid. We selected four PSAP devices that were technologically strong (i.e. meet many standards a hearing aid might be asked to meet) and one PSAP that was technologically fairly poor (i.e. lots of sound distortion) after an in-house electroacoustic analysis of devices. Our hearing aid was selected because it was a popular choice at a university audiology clinic. Forty-two people completed the speech testing unaided (i.e. with no device) and then with each of the five PSAPs and one hearing aid (order of devices was randomized).
We looked at improvement with the devices from unaided. We found that some PSAPs help people understand speech about as well as a hearing aid in this controlled environment while one PSAP actually hindered participants’ ability to understand speech due to sound distortion – imagine how difficult it can be when listening on a poor cell phone signal.
Dr. Nicholas Reed[/caption]
Nicholas S. Reed, AuD
Instructor | Department of Otolaryngology-Head/Neck Surgery
PhD Candidate | Graduate Training Program in Clinical Investigation
Center on Aging and Health
Johns Hopkins University School of Medicine
Johns Hopkins University Bloomberg School of Public Health
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Hearing Aids are medical devices regulated by the FDA which must be purchased through a licensed individual while personal sound amplification products (PSAPs) are essentially unregulated devices some of which can manipulate and increase sound similar to a hearing aid but cannot market themselves are devices for hearing loss. PSAPs can be purchased online or in the back of a store and are generally less expensive than hearing aids.
We aimed to explore a select group of PSAPs to see if they helped someone with mild to moderate hearing loss improve speech understanding (i.e. ability to repeat back sentences) in the presence of mild background noise (think a lunch crowd at a restaurant) as well as a hearing aid. We selected four PSAP devices that were technologically strong (i.e. meet many standards a hearing aid might be asked to meet) and one PSAP that was technologically fairly poor (i.e. lots of sound distortion) after an in-house electroacoustic analysis of devices. Our hearing aid was selected because it was a popular choice at a university audiology clinic. Forty-two people completed the speech testing unaided (i.e. with no device) and then with each of the five PSAPs and one hearing aid (order of devices was randomized).
We looked at improvement with the devices from unaided. We found that some PSAPs help people understand speech about as well as a hearing aid in this controlled environment while one PSAP actually hindered participants’ ability to understand speech due to sound distortion – imagine how difficult it can be when listening on a poor cell phone signal.
 Peter Carew[/caption]
Peter Carew
Lead author, MCRI PhD student
Clinician
The University of Melbourne
MedicalResearch.com: What is the background for this study?
Response: The age at diagnosis of a congenital hearing loss has dropped over time. This has allowed for earlier fitting of amplification (hearing aids, cochlear implants) and earlier access to education intervention programs, all intended to lessen the impact of hearing loss on development. Much research has focused on the outcomes achieved by children with severe and profound losses, but relatively little attention has been given to milder hearing losses (mild and moderate). Despite this lack of evidence, we are observing children with mild loss being fitted with hearing aids earlier than ever before. From a historical age of fitting not uncommonly at 2 years of age or older, today the largest number of children under 12 months who receive a hearing aid for the first time in Australia have a mild hearing loss in their better hearing ear. To this end, clinical practice may have jumped ahead of the evidence in terms of understanding any benefits children with mild hearing loss receive from having hearing aids earlier.
Peter Carew[/caption]
Peter Carew
Lead author, MCRI PhD student
Clinician
The University of Melbourne
MedicalResearch.com: What is the background for this study?
Response: The age at diagnosis of a congenital hearing loss has dropped over time. This has allowed for earlier fitting of amplification (hearing aids, cochlear implants) and earlier access to education intervention programs, all intended to lessen the impact of hearing loss on development. Much research has focused on the outcomes achieved by children with severe and profound losses, but relatively little attention has been given to milder hearing losses (mild and moderate). Despite this lack of evidence, we are observing children with mild loss being fitted with hearing aids earlier than ever before. From a historical age of fitting not uncommonly at 2 years of age or older, today the largest number of children under 12 months who receive a hearing aid for the first time in Australia have a mild hearing loss in their better hearing ear. To this end, clinical practice may have jumped ahead of the evidence in terms of understanding any benefits children with mild hearing loss receive from having hearing aids earlier.
 Dr. Landegger[/caption]
Lukas Landegger MD
Molecular Neurotology Laboratory (PI Konstantina Stankovic)
Massachusetts Eye and Ear Infirmary
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Genetic hearing loss affects more than 125 million people worldwide and constitutes a major hurdle for language acquisition and child development in general. Technological advances over the last decades, such as cochlear implants, have made it possible for deaf children to partially regain their sense of hearing. However, these devices still have several shortcomings, especially when listeners attempt to understand speech in noise or listen to music.
In establishing Anc80L65 as a reliable vector for gene delivery in the inner ear and releasing the first data demonstrating convincing hearing and vestibular function rescue in mice, we provide a foundation for other researchers interested in assessing the benefits of gene therapy in animal models of human disease.
Dr. Landegger[/caption]
Lukas Landegger MD
Molecular Neurotology Laboratory (PI Konstantina Stankovic)
Massachusetts Eye and Ear Infirmary
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Genetic hearing loss affects more than 125 million people worldwide and constitutes a major hurdle for language acquisition and child development in general. Technological advances over the last decades, such as cochlear implants, have made it possible for deaf children to partially regain their sense of hearing. However, these devices still have several shortcomings, especially when listeners attempt to understand speech in noise or listen to music.
In establishing Anc80L65 as a reliable vector for gene delivery in the inner ear and releasing the first data demonstrating convincing hearing and vestibular function rescue in mice, we provide a foundation for other researchers interested in assessing the benefits of gene therapy in animal models of human disease.
 Dr. Larry Humes[/caption]
Larry Humes, PhD, CCC-A
Department of Speech and Hearing Sciences
Indiana University Bloomington
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: About 40% of adults over the age of 60 have significant hearing loss, yet only about 20% of these older Americans seek help and eventually purchase hearing aids. There have been several national calls for improvements in the accessibility and affordability of hearing health care for adults, especially older adults, including a 2015 report by the President’s Council of Advisors in Science and Technology and a 2016 report by the National Academies of Science, Engineering and Medicine. One strategy in common to both of these recent reports is to make hearing aids available directly to the consumer via over-the-counter service delivery.
This study was a double-blind placebo-controlled randomized clinical trial investigating two different service-delivery approaches, best-practices and over-the-counter, and two different purchase prices for the hearing aids ($600/pair, $3600/pair). For the most part, purchase price had no influence on outcomes. Hearing aids delivered via the best-practices service-delivery model were confirmed to be efficacious, but almost identical positive outcomes were obtained via the over-the-counter service-delivery approach.
Dr. Larry Humes[/caption]
Larry Humes, PhD, CCC-A
Department of Speech and Hearing Sciences
Indiana University Bloomington
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: About 40% of adults over the age of 60 have significant hearing loss, yet only about 20% of these older Americans seek help and eventually purchase hearing aids. There have been several national calls for improvements in the accessibility and affordability of hearing health care for adults, especially older adults, including a 2015 report by the President’s Council of Advisors in Science and Technology and a 2016 report by the National Academies of Science, Engineering and Medicine. One strategy in common to both of these recent reports is to make hearing aids available directly to the consumer via over-the-counter service delivery.
This study was a double-blind placebo-controlled randomized clinical trial investigating two different service-delivery approaches, best-practices and over-the-counter, and two different purchase prices for the hearing aids ($600/pair, $3600/pair). For the most part, purchase price had no influence on outcomes. Hearing aids delivered via the best-practices service-delivery model were confirmed to be efficacious, but almost identical positive outcomes were obtained via the over-the-counter service-delivery approach.
 Dr. Gwenaelle Geleoc[/caption]
Gwenaelle Geleoc, PhD
Assistant Professor
Department of Otolaryngology
F.M. Kirby Neurobiology Center
Children's Hospital and Harvard Medical School
Boston, MA
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: We seek to develop gene therapy to restore auditory and balance function in a mouse model of Usher syndrome. Usher syndrome is a rare genetic disorder which causes deafness, progressive blindness and in some cases balance deficits. We used a novel viral vector developed by Luk Vandenberghe and package gene sequences encoding for Ush1c and applied it to young mice suffering from Usher syndrome. These mice mimic a mutation found in patients of Acadian descent. We assessed recovery of hearing and balance function in young adult mice which had received the treatment. Otherwise deaf and dizzy, we found that the treated mice had recovered hearing down to soft sounds equivalent to a whisper and normal balance function.
Dr. Gwenaelle Geleoc[/caption]
Gwenaelle Geleoc, PhD
Assistant Professor
Department of Otolaryngology
F.M. Kirby Neurobiology Center
Children's Hospital and Harvard Medical School
Boston, MA
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: We seek to develop gene therapy to restore auditory and balance function in a mouse model of Usher syndrome. Usher syndrome is a rare genetic disorder which causes deafness, progressive blindness and in some cases balance deficits. We used a novel viral vector developed by Luk Vandenberghe and package gene sequences encoding for Ush1c and applied it to young mice suffering from Usher syndrome. These mice mimic a mutation found in patients of Acadian descent. We assessed recovery of hearing and balance function in young adult mice which had received the treatment. Otherwise deaf and dizzy, we found that the treated mice had recovered hearing down to soft sounds equivalent to a whisper and normal balance function.