MedicalResearch.com Interview with:
Liliana Sanchez-Gonzalez MD, MPH
Medical Epidemiologist
Dengue Branch – Division of Vector Borne Diseases
Centers for Disease Control and Prevention
San Juan, PR
MedicalResearch.com: What is the background for this study? Would you briefly explain the significance of prion disease?
Response: Prion diseases are neurodegenerative diseases that occur in animals and humans. These diseases are caused by an infectious agent known as a prion. While the accuracy of diagnostic tests using cerebrospinal fluid or brain imaging from living patients has improved greatly in recent years, analysis of brain tissue is still necessary to confirm the diagnosis of these diseases.
[caption id="attachment_55692" align="alignleft" width="300"]
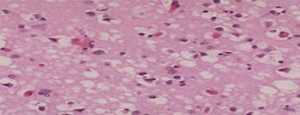
This tissue slide shows sponge-like lesions in the brain tissue of a classic CJD patient.[/caption]
Human prion disease cases are rare, but always fatal. There have been around 500 reported cases annually in the US in recent years. A very small percentage of human prion disease cases are acquired, meaning they are caused by an exposure to the infectious agent from an external source. The most well-known acquired human prion disease is variant Creutzfeldt-Jakob disease (vCJD), which was first described in the United Kingdom in 1996 and linked to consumption of contaminated beef from cattle with the animal prion disease bovine spongiform encephalopathy (BSE, or “mad cow” disease).
The only US state where classic BSE has been reported is Washington, where an infected dairy cow was imported from Canada in 2003. Beef from the slaughtered cow was processed for human consumption, and beef from cattle slaughtered the same day at the involved slaughter plant was recalled. After this incident, the Washington State Department of Health, in collaboration with the US Centers for Disease Control and Prevention and the National Prion Disease Pathology Surveillance Center (NPDPSC), implemented enhanced human prion disease surveillance. All patients with positive results from tests conducted at the NPDPSC are investigated. We present the results of 12 years of human prion disease surveillance, from 2006 to 2017, plus results of surveillance for vCJD through July 2020.


 Dr. Curtis J. Donskey[/caption]
Curtis J. Donskey, MD
Professor of Medicine
Case Western Reserve University
Staff Physician, Infectious Diseases Section,
Louis Stokes Cleveland VA Medical Center
MedicalResearch.com: What is the background for this study?
Response: The goal of the study was to obtain a better understanding of how healthcare-associated pathogens are transmitted. Infection control efforts tend to emphasize hand hygiene and cleaning of high-touch surfaces in patient rooms. However, there is evidence that portable equipment and floors could be underappreciated sources of transmission.
We previously found that a nonpathogenic virus inoculated onto floors in patient rooms spread rapidly to the hands of patients and to surfaces in the room and throughout the ward. This raised concern that pathogens could spread by the same route.
Dr. Curtis J. Donskey[/caption]
Curtis J. Donskey, MD
Professor of Medicine
Case Western Reserve University
Staff Physician, Infectious Diseases Section,
Louis Stokes Cleveland VA Medical Center
MedicalResearch.com: What is the background for this study?
Response: The goal of the study was to obtain a better understanding of how healthcare-associated pathogens are transmitted. Infection control efforts tend to emphasize hand hygiene and cleaning of high-touch surfaces in patient rooms. However, there is evidence that portable equipment and floors could be underappreciated sources of transmission.
We previously found that a nonpathogenic virus inoculated onto floors in patient rooms spread rapidly to the hands of patients and to surfaces in the room and throughout the ward. This raised concern that pathogens could spread by the same route.

 Dr. Batool-Anwar[/caption]
Salma Batool-Anwar, MBBS, MPH
Instructor, Harvard Medical School
Pulmonary and Critical Care, Sleep Medicine
Brigham and Women's Faulkner Hospital
MedicalResearch.com: What is the background for this study?
Response: A well functioning sleep-wake cycle is vital to our health and prevention of chronic diseases.
During previous disaters sleep disturbances have been reported.
When Massachusetts governor declared a state of emergency in March’20, we hypothesized that sleep duration would be adversely affected by covid-19 related lockdown and stress.
The study was approved by the institutional review board and information was collected retrospectively using the electronic medical records.
Dr. Batool-Anwar[/caption]
Salma Batool-Anwar, MBBS, MPH
Instructor, Harvard Medical School
Pulmonary and Critical Care, Sleep Medicine
Brigham and Women's Faulkner Hospital
MedicalResearch.com: What is the background for this study?
Response: A well functioning sleep-wake cycle is vital to our health and prevention of chronic diseases.
During previous disaters sleep disturbances have been reported.
When Massachusetts governor declared a state of emergency in March’20, we hypothesized that sleep duration would be adversely affected by covid-19 related lockdown and stress.
The study was approved by the institutional review board and information was collected retrospectively using the electronic medical records. 

 Mr. Olin[/caption]
Steve Olin
Chief Product Officer
Rally Health, Inc., part of the Optum business of UnitedHealth Grou
MedicalResearch.com: Can you please elaborate on Rally Health’s mission?
Mr. Olin: Our founding mission 10 years ago and still to this day is to put health in the hands of the individual. As a digital health company, we live this mission through our focus in three key areas:
1) Providing digital-first access to care by giving individuals easy-to-use digital tools and support to navigate their health care and take full advantage of their health benefits;
2) Engaging people in their daily health by creating experiences that people enjoy and that inspire them to perform healthy actions, and by giving them access to resources that help them achieve their health goals;
3) Saving people time and money by providing digital tools that help them understand health care costs and guide them to lower-cost, high-quality care options.
Mr. Olin[/caption]
Steve Olin
Chief Product Officer
Rally Health, Inc., part of the Optum business of UnitedHealth Grou
MedicalResearch.com: Can you please elaborate on Rally Health’s mission?
Mr. Olin: Our founding mission 10 years ago and still to this day is to put health in the hands of the individual. As a digital health company, we live this mission through our focus in three key areas:
1) Providing digital-first access to care by giving individuals easy-to-use digital tools and support to navigate their health care and take full advantage of their health benefits;
2) Engaging people in their daily health by creating experiences that people enjoy and that inspire them to perform healthy actions, and by giving them access to resources that help them achieve their health goals;
3) Saving people time and money by providing digital tools that help them understand health care costs and guide them to lower-cost, high-quality care options.
 Dr. Mazzeffi[/caption]
Michael Mazzeffi MD MPH MSc
Associate Professor of Anesthesiology
Division Chief Anesthesiology Critical Care Medicine
Medical Director Rapid Response Team
MedicalResearch.com: What is the background for this study?
Response: We have known for some time that COVID19 is characterized by hypercoagulability or excess blood clotting. In fact, the incidence of blood clots in the lungs (pulmonary emboli) is as high 20% and is two to three times more common in COVID19 than in severe influenza. Further, autopsies of patients who died from COVID19 have shown that endothelial cells (cells that line the blood vessels) are damaged and that "micro clots" form in multiple organs. Together, these findings strongly suggest that excess blood clotting and endothelial cell dysfunction are defining features of severe COVID19.
For several months, my colleagues and I have been interested in whether aspirin might improve outcomes in patients with severe COVID19. In prior observational research studies, aspirin was found to be protective in patients with severe lung injury. The general idea is that aspirin reduces platelet aggregates in the lung and this improves outcome. Unfortunately, in a prior randomized controlled study (LIPS-A) aspirin was not shown to reduce the incidence of acute respiratory distress syndrome. Nevertheless, COVID19 has unique features that make aspirin more likely to be effective. Mainly COVID19 is associated with hypercoagulability to a greater degree than in other viral illnesses.
Dr. Mazzeffi[/caption]
Michael Mazzeffi MD MPH MSc
Associate Professor of Anesthesiology
Division Chief Anesthesiology Critical Care Medicine
Medical Director Rapid Response Team
MedicalResearch.com: What is the background for this study?
Response: We have known for some time that COVID19 is characterized by hypercoagulability or excess blood clotting. In fact, the incidence of blood clots in the lungs (pulmonary emboli) is as high 20% and is two to three times more common in COVID19 than in severe influenza. Further, autopsies of patients who died from COVID19 have shown that endothelial cells (cells that line the blood vessels) are damaged and that "micro clots" form in multiple organs. Together, these findings strongly suggest that excess blood clotting and endothelial cell dysfunction are defining features of severe COVID19.
For several months, my colleagues and I have been interested in whether aspirin might improve outcomes in patients with severe COVID19. In prior observational research studies, aspirin was found to be protective in patients with severe lung injury. The general idea is that aspirin reduces platelet aggregates in the lung and this improves outcome. Unfortunately, in a prior randomized controlled study (LIPS-A) aspirin was not shown to reduce the incidence of acute respiratory distress syndrome. Nevertheless, COVID19 has unique features that make aspirin more likely to be effective. Mainly COVID19 is associated with hypercoagulability to a greater degree than in other viral illnesses. 
 Dr. Leaf[/caption]
David E. Leaf, MD, MMSc, FASN
Assistant Professor of Medicine, Harvard Medical School
Director of Clinical and Translational Research in Acute Kidney Injury
Division of Renal Medicine, Brigham and Women's Hospital
MedicalResearch.com: What is the background for this study?
Response: The data for this study were derived from a multicenter cohort study of over 4,000 critically ill patients with COVID-19 admitted to ICUs at 68 sites across the US, as part of the Study of the Treatment and Outcomes in Critically Ill Patients with COVID-19 (STOP-COVID). STOP-COVID was initiated by David E. Leaf, MD, MMSc and Shruti Gupta, MD, MPH, from the Division of Renal Medicine at Brigham and Women’s Hospital and Harvard Medical School. It was initiated in March, 2020 as an unfunded, grassroots network, and now includes over 400 collaborators from 68 sites across the US.
Using this data, we used a ‘target trial emulation’ approach to examine whether early administration of the monoclonal antibody, tocilizumab, reduces mortality in critically ill patients with COVID-19. Target trial emulation, a novel method of analyzing observational data, is the idea of simulating a randomized control trial to reduce bias.
Dr. Leaf[/caption]
David E. Leaf, MD, MMSc, FASN
Assistant Professor of Medicine, Harvard Medical School
Director of Clinical and Translational Research in Acute Kidney Injury
Division of Renal Medicine, Brigham and Women's Hospital
MedicalResearch.com: What is the background for this study?
Response: The data for this study were derived from a multicenter cohort study of over 4,000 critically ill patients with COVID-19 admitted to ICUs at 68 sites across the US, as part of the Study of the Treatment and Outcomes in Critically Ill Patients with COVID-19 (STOP-COVID). STOP-COVID was initiated by David E. Leaf, MD, MMSc and Shruti Gupta, MD, MPH, from the Division of Renal Medicine at Brigham and Women’s Hospital and Harvard Medical School. It was initiated in March, 2020 as an unfunded, grassroots network, and now includes over 400 collaborators from 68 sites across the US.
Using this data, we used a ‘target trial emulation’ approach to examine whether early administration of the monoclonal antibody, tocilizumab, reduces mortality in critically ill patients with COVID-19. Target trial emulation, a novel method of analyzing observational data, is the idea of simulating a randomized control trial to reduce bias. 
 Dr. Meyers[/caption]
Craig Meyers, PhD
Department of Microbiology and Immunology
Pennsylvania State College of Medicine
Hershey, PA
MedicalResearch.com: What is the background for this study?
Response: As nasal and oral cavities are major points of entry and transmission for human coronaviruses our team of physicians and scientists (Craig Meyers, Janice Milici, Samina Alam, David Quillen, David Goldenberg and Rena Kass of Penn State College of Medicine and Richard Robison of Brigham Young University) were interested in testing common over-the-counter oral antiseptics and mouthwashes for their efficacy to inactivate infectious human coronavirus, which is structurally similar to SARS-CoV-2, the virus that causes COVID-19. While we wait for a vaccine for COVID-19 to be developed, methods to reduce transmission are needed. We chose products that are readily available and often already part of people’s daily routines.
Dr. Meyers[/caption]
Craig Meyers, PhD
Department of Microbiology and Immunology
Pennsylvania State College of Medicine
Hershey, PA
MedicalResearch.com: What is the background for this study?
Response: As nasal and oral cavities are major points of entry and transmission for human coronaviruses our team of physicians and scientists (Craig Meyers, Janice Milici, Samina Alam, David Quillen, David Goldenberg and Rena Kass of Penn State College of Medicine and Richard Robison of Brigham Young University) were interested in testing common over-the-counter oral antiseptics and mouthwashes for their efficacy to inactivate infectious human coronavirus, which is structurally similar to SARS-CoV-2, the virus that causes COVID-19. While we wait for a vaccine for COVID-19 to be developed, methods to reduce transmission are needed. We chose products that are readily available and often already part of people’s daily routines.

 Dr. Kriner[/caption]
Douglas L. Kriner, PhD
The Clinton Rossiter Professor in American Institutions
Department of Government
Cornell University
MedicalResearch.com: What is the background for this study?
Response: When a safe and effective vaccine for COVID-19 reaches the market, the world will not change overnight. Rather, government and public health individuals will have to develop a comprehensive plan to distribute the vaccine and to convince potentially wary Americans to take it.
Our study examined the influence of both specific vaccine characteristics and the politics surrounding it on public willingness to vaccinate. Both matter in important ways. For example, efficacy is unsurprisingly a major driver of public opinion; Americans are more willing to take a vaccine that is more efficacious.
Dr. Kriner[/caption]
Douglas L. Kriner, PhD
The Clinton Rossiter Professor in American Institutions
Department of Government
Cornell University
MedicalResearch.com: What is the background for this study?
Response: When a safe and effective vaccine for COVID-19 reaches the market, the world will not change overnight. Rather, government and public health individuals will have to develop a comprehensive plan to distribute the vaccine and to convince potentially wary Americans to take it.
Our study examined the influence of both specific vaccine characteristics and the politics surrounding it on public willingness to vaccinate. Both matter in important ways. For example, efficacy is unsurprisingly a major driver of public opinion; Americans are more willing to take a vaccine that is more efficacious.
 Dr. KantersA[/caption]
Response: A watershed moment for the fight against HIV was the antiretroviral treatment (ART) scale-up that made HIV treatments available around the world. While HIV activism led to its initiation, two key ingredients to the ART scale-up were the advent of a once-daily single-pill HIV treatment and the creation of the World Health Organization (WHO) clinical guidelines for treatment and prevention of HIV. The HIV treatment in question combines three drugs in a single pill and centers around a drug called efavirenz.
The WHO guidelines use a public health framework, which is to say that it uses a treatment algorithm that is both equitable and simple enough to allow some task-shifting to less specialized workers. As such, the guidelines suggest a single preferred treatment for people initiating HIV treatment. While resource rich countries can use a personalized medicine approach, many settings where HIV is endemic cannot.
In 2015, our review found strong evidence that a newer HIV drug, called dolutegravir, was better than efavirenz in respect to efficacy, tolerability and safety; however, there was not enough evidence to support its use in key populations, such as people with HIV-tuberculosis co-infections and pregnant women. For this and other reasons, the WHO could not recommend its use as the preferred treatment at initiation.
Since then, we have continued to dynamically assess the evidence to determine the best treatment to have as the preferred ART for first-time HIV treatment. This is the culmination of 6 years of work and its findings have helped the WHO change its recommended preferred first-line therapy from an efavirenz-based ART to a dolutegravir-based ART.
Dr. KantersA[/caption]
Response: A watershed moment for the fight against HIV was the antiretroviral treatment (ART) scale-up that made HIV treatments available around the world. While HIV activism led to its initiation, two key ingredients to the ART scale-up were the advent of a once-daily single-pill HIV treatment and the creation of the World Health Organization (WHO) clinical guidelines for treatment and prevention of HIV. The HIV treatment in question combines three drugs in a single pill and centers around a drug called efavirenz.
The WHO guidelines use a public health framework, which is to say that it uses a treatment algorithm that is both equitable and simple enough to allow some task-shifting to less specialized workers. As such, the guidelines suggest a single preferred treatment for people initiating HIV treatment. While resource rich countries can use a personalized medicine approach, many settings where HIV is endemic cannot.
In 2015, our review found strong evidence that a newer HIV drug, called dolutegravir, was better than efavirenz in respect to efficacy, tolerability and safety; however, there was not enough evidence to support its use in key populations, such as people with HIV-tuberculosis co-infections and pregnant women. For this and other reasons, the WHO could not recommend its use as the preferred treatment at initiation.
Since then, we have continued to dynamically assess the evidence to determine the best treatment to have as the preferred ART for first-time HIV treatment. This is the culmination of 6 years of work and its findings have helped the WHO change its recommended preferred first-line therapy from an efavirenz-based ART to a dolutegravir-based ART.  Dr. Profeta[/caption]
Paola Profeta, PhD
Professor of Public Economics, Department of Social and Political Sciences
Bocconi University
Director, Msc Politics and Policy Analysis, Bocconi University
Coordinator, Dondena Gender Initiative, Dondena Research Center
President, European Public Choice Society
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: We interview more than 20000 men and women in 8 OECD countries in two periods during the lockdown.
Using two waves from 8 OECD countries, we find that women are more likely to perceive the pandemic as a very serious health problem, to agree with restraining measures and to comply with public health rules, such as using facemasks. This gender differences are less strong for married individuals and for individuals who have been directly exposed to COVID, for instance by knowing someone who was infected.
Dr. Profeta[/caption]
Paola Profeta, PhD
Professor of Public Economics, Department of Social and Political Sciences
Bocconi University
Director, Msc Politics and Policy Analysis, Bocconi University
Coordinator, Dondena Gender Initiative, Dondena Research Center
President, European Public Choice Society
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: We interview more than 20000 men and women in 8 OECD countries in two periods during the lockdown.
Using two waves from 8 OECD countries, we find that women are more likely to perceive the pandemic as a very serious health problem, to agree with restraining measures and to comply with public health rules, such as using facemasks. This gender differences are less strong for married individuals and for individuals who have been directly exposed to COVID, for instance by knowing someone who was infected.
 Shane Riddell[/caption]
Shane Riddell MSc
CSIRO—Australian Animal Health Laboratory
Geelong, Australia
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: While it is generally considered that SARS-CoV-2 is spread via aerosol and respiratory droplets, we still need to investigate how much of a role fomites play in transmission.
Understanding the risk first requires you to know how long the virus can survive on a surface. We therefore wanted to assess how long the virus would remain viable on various common surfaces such as stainless steel, glass and banknotes. We found that, under controlled conditions, we could recover infectious virus at 28 days for all non-porous surfaces at 20 degrees Celsius. When the temperature was raised to 40 degrees Celsius, SARS-CoV-2 only remained viable for 24hrs on most surfaces.
Shane Riddell[/caption]
Shane Riddell MSc
CSIRO—Australian Animal Health Laboratory
Geelong, Australia
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: While it is generally considered that SARS-CoV-2 is spread via aerosol and respiratory droplets, we still need to investigate how much of a role fomites play in transmission.
Understanding the risk first requires you to know how long the virus can survive on a surface. We therefore wanted to assess how long the virus would remain viable on various common surfaces such as stainless steel, glass and banknotes. We found that, under controlled conditions, we could recover infectious virus at 28 days for all non-porous surfaces at 20 degrees Celsius. When the temperature was raised to 40 degrees Celsius, SARS-CoV-2 only remained viable for 24hrs on most surfaces.


 Dr. Nagata, MD[/caption]
Jason Nagata, MD, MSc
Assistant Professor of Pediatrics
University of California, San Francisco
San Francisco, California, USA
MedicalResearch.com: What is the background for this study?
Response: During the COVID-19 pandemic, food insecurity is expected to rise given economic uncertainty and job losses. Vulnerable and marginalized populations are disproportionately affected by both COVID-19 and food insecurity.
MedicalResearch.com: What are the main findings?
Response: In this perspective, we argue that food insecurity and COVID-19 can exacerbate one another via bidirectional links. Experiencing food insecurity can lead to nutritional deficiencies and weakened host defenses, increasing susceptibility to COVID-19 infection. Food insecurity is also associated with chronic medical conditions which may lead to a higher risk of severe COVID-19 illness.
Conversely, people with COVID-19 may not be able to work, generate income, or procure food while quarantined, which may worsen food insecurity.
Dr. Nagata, MD[/caption]
Jason Nagata, MD, MSc
Assistant Professor of Pediatrics
University of California, San Francisco
San Francisco, California, USA
MedicalResearch.com: What is the background for this study?
Response: During the COVID-19 pandemic, food insecurity is expected to rise given economic uncertainty and job losses. Vulnerable and marginalized populations are disproportionately affected by both COVID-19 and food insecurity.
MedicalResearch.com: What are the main findings?
Response: In this perspective, we argue that food insecurity and COVID-19 can exacerbate one another via bidirectional links. Experiencing food insecurity can lead to nutritional deficiencies and weakened host defenses, increasing susceptibility to COVID-19 infection. Food insecurity is also associated with chronic medical conditions which may lead to a higher risk of severe COVID-19 illness.
Conversely, people with COVID-19 may not be able to work, generate income, or procure food while quarantined, which may worsen food insecurity.

 Dr. Garg[/caption]
Dr. Madhur Garg, MD MBA
Clinical director, Radiation Oncology
Montefiore Health System and Professor
Departments of Otorhinolaryngology - Head & Neck Surgery - and Urology
Albert Einstein College of Medicine
MedicalResearch.com: What is the background for this study?
Response: The Bronx was hit particularly hard with Covid-19 - making up one of the highest per capita cases and deaths in the country. Montefiore Health System and Albert Einstein College of Medicine, care for a large population of ethnic minorities (non-Hispanic Black and Hispanic individuals make up 65% of our patient population).
Dr. Garg[/caption]
Dr. Madhur Garg, MD MBA
Clinical director, Radiation Oncology
Montefiore Health System and Professor
Departments of Otorhinolaryngology - Head & Neck Surgery - and Urology
Albert Einstein College of Medicine
MedicalResearch.com: What is the background for this study?
Response: The Bronx was hit particularly hard with Covid-19 - making up one of the highest per capita cases and deaths in the country. Montefiore Health System and Albert Einstein College of Medicine, care for a large population of ethnic minorities (non-Hispanic Black and Hispanic individuals make up 65% of our patient population).









