
Annals Internal Medicine
11 Mar Physicians, PAs and Nurse Practitioners Provide Similar Amount of Low Value Care
MedicalResearch.com Interview with: [caption id="attachment_32850" align="alignleft" width="200"] Dr. John N. Mafi[/caption]
John N. Mafi, MD, MPH
Division of General Internal Medicine and Health Services Research
Department of Medicine, Ronald Reagan UCLA Medical Center
Los Angeles, CA
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Our country has a primary care physician shortage. Some have advocated that we expand the scope of practice for nurse practitioners and physician assistants to help alleviate this problem and improve access to primary care. But a 2013 study in the New England Journal of Medicine found that a large number of physicians believed that nurse practitioners provided lower value care when compared with physicians. We decided to put that belief to the test. We studied 29,000 U.S. patients who saw either a nurse practitioner, physician assistant, or physician in the primary care setting for common conditions, and we compared the rate of low-value or unnecessary services—for example, unnecessary antibiotics for the common cold, or MRI for low back pain, or a CT scan for headache. Things that don’t help patients and may harm.
We found no difference in the rates of low value services between nurse practitioners, physician assistants, and physicians. In other words, they did equivalent amounts of inappropriate or bad care.
Dr. John N. Mafi[/caption]
John N. Mafi, MD, MPH
Division of General Internal Medicine and Health Services Research
Department of Medicine, Ronald Reagan UCLA Medical Center
Los Angeles, CA
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Our country has a primary care physician shortage. Some have advocated that we expand the scope of practice for nurse practitioners and physician assistants to help alleviate this problem and improve access to primary care. But a 2013 study in the New England Journal of Medicine found that a large number of physicians believed that nurse practitioners provided lower value care when compared with physicians. We decided to put that belief to the test. We studied 29,000 U.S. patients who saw either a nurse practitioner, physician assistant, or physician in the primary care setting for common conditions, and we compared the rate of low-value or unnecessary services—for example, unnecessary antibiotics for the common cold, or MRI for low back pain, or a CT scan for headache. Things that don’t help patients and may harm.
We found no difference in the rates of low value services between nurse practitioners, physician assistants, and physicians. In other words, they did equivalent amounts of inappropriate or bad care.
21 Feb Tele-Rehabilitation Can Improve Physical Function In Chronic Knee Pain Patients
MedicalResearch.com Interview with: Rachel Nelligan, BPhysio Physiotherapist & Research Physiotherapist Department of Physiotherapy | Centre for Health, Exercise and Sports Medicine The University of Melbourne Victoria Australia MedicalResearch.com: What is the background for this study? Response: This novel study investigated the efficacy of an internet delivered model of service delivery that combined online education, Skype delivered exercise physiotherapy and an Internet-based interactive pain coping skills training program for people with persistent knee pain. Osteoarthritis, the leading cause of chronic knee pain and disability globally, has a significant individual, societal and economic burden. On an individual level knee osteoarthritis causes loss of function, reduced quality of life, and psychological distress. Clinical guidelines recommend adoption of a biopsychosocial approach to management which should include nondrug, nonsurgical treatments. Specifically exercise, education and psychological interventions (including pain coping skills training (PCST)) that foster self-management are recommended. Evidence identifies that many knee OA sufferers are not receiving adequate management due in part to challenges of accessing these effective treatments. There is an urgent need for new models of health service delivery to rectify this. Tele-rehabilitation is growing in acceptance as an effective, time efficient and convenient means for people to access effective health interventions. In knee OA internet delivered interventions specifically remotely delivered physiotherapy exercise using specialised tele-rehabilitation equipment and an Internet-based interactive PCST program (PainCOACH), designed to translate key therapeutic elements of clinician-delivered face-to-face PCST, have shown improved patient outcomes. Prior to this study the combination of these two internet-based treatments has not been investigated.08 Feb Smokers Who Switch Completely To E-Cigs Reduce Their Exposure to Toxins
Posted at 01:41h
in Annals Internal Medicine, Author Interviews, Smoking, Tobacco, Tobacco Research, Toxin Research
MedicalResearch.com Interview with: Dr Lion Shahab MA (Oxon) MSc MSc PhD CPsychol AFBPsS PGCLTHE Senior Lecturer in Health Psychology Department of Behavioural Science and Health University College London London MedicalResearch.com: What is the background for this study? What are the main findings? Response: To date most studies on e-cigs have either looked at the product itself, i.e. analysed...
01 Feb Exposure to Violence, Psychological Distress, and Gun Carrying Among Male Adolescents
MedicalResearch.com Interview with: Joan A. Reid, Ph.D., LMHC Assistant Professor Criminology Program DAV 266 University of South Florida St. Petersburg MedicalResearch.com: What is the background for this study? What are the main findings? Response: Firearm-associated homicide and suicide are leading causes of death among American youth (i.e., 10-24 years old), with disproportionately high rates observed among male youth of color. Notably, gun violence and psychological problems are often conflated in public discourse regarding gun violence and prevention. However, few studies have assessed the impact of exposure to violence, either as a witness or a victim, when exploring the association between gun-carrying behavior and psychological distress.30 Jan Medical Residents Spend More Time Working on Electronic Medical Records than With Patients
MedicalResearch.com Interview with: Dresse Nathalie Wenger Cheffe de clinique FMH médecine interne Département de Médecine Interne CHUV - Lausanne MedicalResearch.com: What is the background for this study? Response: The structure of a residents’ working day dramatically changed during the last decades (limitation of working hours per week, wide implementation of electronic medical records (EMR), and growing volume of clinical data and administrative tasks), especially in internal medicine with increasing complexity of patients. Electronic Medical Records (EMR) have some positive effects but negative effects have been also described ie more time writing notes, more administrative works, and less time for communication between physicians and patients. Few time motion studies have been published about the resident's working day in Internal Medicine: the impact of the computer, and what really do the residents do during their work, especially the time spent with the patient versus the computer, as now the EMRs are widely implemented. Previous studies have been mostly performed in the US, so we decided to conduct one observational and objective study in Europe.13 Jan Breast and Prostate Cancer Screenings Have Similar Potential for OverDiagnosis
Posted at 00:20h
in Annals Internal Medicine, Author Interviews, Breast Cancer, Cancer Research, Prostate Cancer
MedicalResearch.com Interview with:
Karsten Juhl Jørgensen, MD, Dr. MedSci
The Nordic Cochrane Centre
Rigshospitalet, Copenhagen
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Our systematic Cochrane review of the original randomised breast screening trials showed substantial conflict between their estimates of the benefit. Some trials showed a large benefit, others none or a small benefit. This difference was related to the design of the trials.
The most optimistic trials were those with suboptimal randomisation.
The main findings of our current study support those of the most rigorously performed randomised trials: breast screening does not fulfill its fundamental premise, which is to reduce the occurrence of late stage disease. This means a mortality reduction is unlikely and that use of less invasive surgery due to breast screening is also unlikely.
However, we did find very substantial increases in early stage breast cancer, which persisted over our 17 year observation period. This means that breast screening likely leads to substantial overdiagnosis of breast cancers that would otherwise not have caused health problems during a woman’s lifetime. We estimate that 1 in 3 breast cancers detected in a screened population is likely overdiagnosed.
11 Jan Little Evidence Pay-For-Performance Improves Patient Outcomes
MedicalResearch.com Interview with: [caption id="attachment_31055" align="alignleft" width="200"] Dr. Devan Kansagara[/caption]
Devan Kansagara MD, MCR
Associate Professor of Medicine
Oregon Health and Science University
Director, Evidence-based Synthesis Program, Portland VA Medical Center
Staff Physician, Portland VA Medical Center
MedicalResearch.com: What is the background for this study?
Response: Historically, the US health care system has been dominated by a fee-for-service payment structure in which health care providers are paid for discrete procedures and visits regardless of care quality. Pay for performance programs are part of the move towards value-based care. They tie a portion of payments to individual health care providers, institutions, or health care systems to performance on a discrete set of measures of health care quality.
In theory, these programs are meant to encourage the right care at the right time and thereby improve the health of the patient population. Over the last decade, many studies in and outside the US have examined whether or not, in fact, these programs do result in improved care, reduced cost, and improved patient health. Our study is a systematic review of this literature.
Dr. Devan Kansagara[/caption]
Devan Kansagara MD, MCR
Associate Professor of Medicine
Oregon Health and Science University
Director, Evidence-based Synthesis Program, Portland VA Medical Center
Staff Physician, Portland VA Medical Center
MedicalResearch.com: What is the background for this study?
Response: Historically, the US health care system has been dominated by a fee-for-service payment structure in which health care providers are paid for discrete procedures and visits regardless of care quality. Pay for performance programs are part of the move towards value-based care. They tie a portion of payments to individual health care providers, institutions, or health care systems to performance on a discrete set of measures of health care quality.
In theory, these programs are meant to encourage the right care at the right time and thereby improve the health of the patient population. Over the last decade, many studies in and outside the US have examined whether or not, in fact, these programs do result in improved care, reduced cost, and improved patient health. Our study is a systematic review of this literature.
21 Dec No Association Between Length of Red Blood Cell Storage and Mortality
MedicalResearch.com Interview with: Märit Halmin, MD, PhD student Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden MedicalResearch.com: What is the background for this study? Response: During recent years the possible negative effects among recipients of stored red blood cells have been investigated. Despite a large number of studies, including four randomized trials, no consensus exists. We therefore performed the hitherto largest register based cohort study of transfused patients, assessing the association between length of storage of red blood cells and mortality. Our design allowed for detection of small but still clinically significant effect, if such exists.19 Dec How Strong is the Scientific Basis of Sugar Intake Guidelines?
MedicalResearch.com Interview with: [caption id="attachment_30649" align="alignleft" width="150"] Dr. Bradley Johnston[/caption]
Bradley C. Johnston, PhD
Prevention Lab, Child Health Evaluative Sciences, The Hospital for Sick Children Research Institute
Peter Gilgan Centre for Research and Learning
Toronto, Ontario
MedicalResearch.com: What is the background for this study?
Response: I am scientist at The Hospital for Sick Children and a professor of clinical epidemiology at the University of Toronto and McMaster University in Canada. I have a particular interest in research methodology and preventive medicine. As a research methodologist I am interested in how researchers get to their conclusions. In particular I am interested in the “uncertainty” in estimated treatment or exposure effects.
Many guidelines have methodological issues but it was suspected that the nutritional guidelines were especially problematic. Our study in Annals of Internal Medicine set out to document the issues systematically with respect to sugar intake recommendations from authoritative guidelines.
Dr. Bradley Johnston[/caption]
Bradley C. Johnston, PhD
Prevention Lab, Child Health Evaluative Sciences, The Hospital for Sick Children Research Institute
Peter Gilgan Centre for Research and Learning
Toronto, Ontario
MedicalResearch.com: What is the background for this study?
Response: I am scientist at The Hospital for Sick Children and a professor of clinical epidemiology at the University of Toronto and McMaster University in Canada. I have a particular interest in research methodology and preventive medicine. As a research methodologist I am interested in how researchers get to their conclusions. In particular I am interested in the “uncertainty” in estimated treatment or exposure effects.
Many guidelines have methodological issues but it was suspected that the nutritional guidelines were especially problematic. Our study in Annals of Internal Medicine set out to document the issues systematically with respect to sugar intake recommendations from authoritative guidelines.
12 Dec Access To Two Different Health Care Systems Can Lead To Dangerous Presciption Combinations
Posted at 22:06h
in Alzheimer's - Dementia, Annals Internal Medicine, Author Interviews, Critical Care - Intensive Care - ICUs, Health Care Systems, University of Pittsburgh
MedicalResearch.com Interview with:
[caption id="attachment_30462" align="alignleft" width="144"] Dr. Joshua Thorpe[/caption]
Joshua M. Thorpe, PhD, MPH
From the Center for Health Equity Research and Promotion
Veterans Affairs Pittsburgh Healthcare System
Pittsburgh Pennsylvania, and
Center for Health Services Research in Primary Care
Department of Pharmacy and Therapeutics
University of Pittsburgh School of Pharmacy
MedicalResearch.com: What is the background for this study?
Response: Care coordination for persons with dementia is challenging for health care systems under the best of circumstances. These coordination challenges are exacerbated in Medicare-eligible veterans who receive care through both Medicare and the Department of Veterans Affairs (VA). Recent Medicare and VA policy changes (e.g., Medicare Part D, Veteran’s Choice Act) expand veterans’ access to providers outside the VA. While access to care may be improved, seeking care across multiple health systems may disrupt care coordination and increase the risk of unsafe prescribing - particularly in veterans with dementia. To see how expanded access to care outside the VA might influence medication safety for veterans with dementia, we studied prescribing safety in Veterans who qualified for prescriptions through the VA as well as through the Medicare Part D drug benefit.
Dr. Joshua Thorpe[/caption]
Joshua M. Thorpe, PhD, MPH
From the Center for Health Equity Research and Promotion
Veterans Affairs Pittsburgh Healthcare System
Pittsburgh Pennsylvania, and
Center for Health Services Research in Primary Care
Department of Pharmacy and Therapeutics
University of Pittsburgh School of Pharmacy
MedicalResearch.com: What is the background for this study?
Response: Care coordination for persons with dementia is challenging for health care systems under the best of circumstances. These coordination challenges are exacerbated in Medicare-eligible veterans who receive care through both Medicare and the Department of Veterans Affairs (VA). Recent Medicare and VA policy changes (e.g., Medicare Part D, Veteran’s Choice Act) expand veterans’ access to providers outside the VA. While access to care may be improved, seeking care across multiple health systems may disrupt care coordination and increase the risk of unsafe prescribing - particularly in veterans with dementia. To see how expanded access to care outside the VA might influence medication safety for veterans with dementia, we studied prescribing safety in Veterans who qualified for prescriptions through the VA as well as through the Medicare Part D drug benefit.
15 Nov Immunotherapy Tofacitinib Can Halt Alopecia Areata
MedicalResearch.com Interview with: Dr. Morton Scheinberg, MD, PhD From Hospital Israelita Albert Einstein and Hospital AACD, São Paulo, and Clinica Dermatosineida, Maringa, Parana, Brazil. MedicalResearch.com: What is the background for this study? What are the main findings? Response: That universal hair loss associated with a localized autoimmune reaction on the cells involved with the hair follicles can be halted with tofacitinib.27 Sep Study Supports Routine Colon Cancer Screening Through Age 75, With Individualized Decisions Afterwards
Posted at 19:48h
in Annals Internal Medicine, Author Interviews, Brigham & Women's - Harvard, Colon Cancer, Geriatrics
MedicalResearch.com Interview with:
[caption id="attachment_28323" align="alignleft" width="124"] Dr. Xabier Garcia-De-Albeniz[/caption]
Xabier Garcia-De-Albeniz MD PhD
Research Associate
Department of Epidemiology
Harvard T.H. Chan School of Public Health
Mongan Institute for Health Policy
Massachusetts General Hospital
MedicalResearch.com: What is the background for this study?
Response: Randomized controlled trials are considered the gold standard to inform health care delivery. Unfortunately, no randomized controlled trials of screening colonoscopy have been completed. Ongoing trials exclude persons aged 75 or older, and will not have mature results before 2025. However, healthy persons older than 75 may live long enough to benefit from colorectal cancer (CRC) screening. The Medicare program reimburses screening colonoscopy without an upper age limit since the year 2001. We used the extensive experience of Medicare beneficiaries to evaluate the effectiveness and safety of screening colonoscopy.
Dr. Xabier Garcia-De-Albeniz[/caption]
Xabier Garcia-De-Albeniz MD PhD
Research Associate
Department of Epidemiology
Harvard T.H. Chan School of Public Health
Mongan Institute for Health Policy
Massachusetts General Hospital
MedicalResearch.com: What is the background for this study?
Response: Randomized controlled trials are considered the gold standard to inform health care delivery. Unfortunately, no randomized controlled trials of screening colonoscopy have been completed. Ongoing trials exclude persons aged 75 or older, and will not have mature results before 2025. However, healthy persons older than 75 may live long enough to benefit from colorectal cancer (CRC) screening. The Medicare program reimburses screening colonoscopy without an upper age limit since the year 2001. We used the extensive experience of Medicare beneficiaries to evaluate the effectiveness and safety of screening colonoscopy.
14 Sep Three Criteria To Identify Out-of-Hospital Cardiac Arrest Patients With No Chance of Survival
MedicalResearch.com Interview with: [caption id="attachment_27901" align="alignleft" width="150"] Prof. Xavier Jouven[/caption]
Prof. Xavier Jouven
Service de Cardiologie
Hôpital Européen Georges Pompidou
Paris
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: There are many cardiac arrests (around 300 000 per year in United States). The possibility to collect organs from a certain proportion of those cardiac arrests represents an important opportunity to fill the gap of the organ shortage.
It is absolutely mandatory to identify patients with no chance of survival. This study showed 3 criteria which allow this early identification. Several thousands of patients die every year waiting for organ transplantation.
Prof. Xavier Jouven[/caption]
Prof. Xavier Jouven
Service de Cardiologie
Hôpital Européen Georges Pompidou
Paris
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: There are many cardiac arrests (around 300 000 per year in United States). The possibility to collect organs from a certain proportion of those cardiac arrests represents an important opportunity to fill the gap of the organ shortage.
It is absolutely mandatory to identify patients with no chance of survival. This study showed 3 criteria which allow this early identification. Several thousands of patients die every year waiting for organ transplantation.
16 Aug Live Nasal and Injectable Flu Vaccines Had Similar Effectiveness in Pediatric Study
Posted at 18:25h
in Annals Internal Medicine, Author Interviews, Flu - Influenza, Pediatrics, Vaccine Studies
MedicalResearch.com Interview with:
[caption id="attachment_26888" align="alignleft" width="150"] Dr. Mark Loeb[/caption]
Dr. Mark Loeb
BSc (McGill), MD (McGill), MSc (McMaster), FRCPC
Professor, Department of Pathology and Molecular Medicine
Joint Member, Dept of Clinical Epidemiology & Biostatistics
Division Director, Infectious Diseases, McMaster University
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: The background for this study is that in the U.S, the Advisory Committee on Immunization Practices (ACIP), the committee that advises the CDC on vaccination policy, decided this June not to recommend LAIV (nasal live vaccine) for children. This is because of non-randomized studies conducted in the U.S suggesting that the vaccine was ineffective. This was an unprecedented decision in influenza vaccine policy making for children.
Our study, a randomized, blinded, controlled trial, which is the most rigorous type of study design, conducted over 3 years (2012-13, 2013-2014, 2014-2015 influenza seasons), showed in fact very similar protection for children and their communities for the live and inactivated vaccines. We conducted the study in the Hutterite community of Western Canada which allowed us to compare the effect of the vaccines in entire communities. That is, we were able to study the direct effect and the indirect effect of these vaccines.
Dr. Mark Loeb[/caption]
Dr. Mark Loeb
BSc (McGill), MD (McGill), MSc (McMaster), FRCPC
Professor, Department of Pathology and Molecular Medicine
Joint Member, Dept of Clinical Epidemiology & Biostatistics
Division Director, Infectious Diseases, McMaster University
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: The background for this study is that in the U.S, the Advisory Committee on Immunization Practices (ACIP), the committee that advises the CDC on vaccination policy, decided this June not to recommend LAIV (nasal live vaccine) for children. This is because of non-randomized studies conducted in the U.S suggesting that the vaccine was ineffective. This was an unprecedented decision in influenza vaccine policy making for children.
Our study, a randomized, blinded, controlled trial, which is the most rigorous type of study design, conducted over 3 years (2012-13, 2013-2014, 2014-2015 influenza seasons), showed in fact very similar protection for children and their communities for the live and inactivated vaccines. We conducted the study in the Hutterite community of Western Canada which allowed us to compare the effect of the vaccines in entire communities. That is, we were able to study the direct effect and the indirect effect of these vaccines.
19 Jul Breast Density Interpretation Varies Among Radiologists
MedicalResearch.com Interview with: Brian L. Sprague, PhD
Assistant Professor
Department of Surgery
Assistant Professor
Department of Biochemistry
University of Vermont
MedicalResearch.com: What is the background for this study?
Response: Having dense breasts makes mammography more difficult to interpret and is also an independent risk factor for developing breast cancer. About half of all U.S. states require that information on the density of a woman's breasts be made available to her after a mammogram, and in some states the report must also inform such women that there are additional tests, such as breast magnetic resonance imaging (MRI), that may detect breast cancer in women who have dense breasts and normal mammograms.
Such laws are controversial because of the large number of women affected (around 40% of women aged 40-74) and due to a lack of consensus in the medical community regarding the benefits and harms of supplemental screening strategies. An additional concern is the subjective nature of breast density assessment, which is based on the Breast Imaging Reporting and Data System (BI-RADS) that provides four possible categories for breast density.
Brian L. Sprague, PhD
Assistant Professor
Department of Surgery
Assistant Professor
Department of Biochemistry
University of Vermont
MedicalResearch.com: What is the background for this study?
Response: Having dense breasts makes mammography more difficult to interpret and is also an independent risk factor for developing breast cancer. About half of all U.S. states require that information on the density of a woman's breasts be made available to her after a mammogram, and in some states the report must also inform such women that there are additional tests, such as breast magnetic resonance imaging (MRI), that may detect breast cancer in women who have dense breasts and normal mammograms.
Such laws are controversial because of the large number of women affected (around 40% of women aged 40-74) and due to a lack of consensus in the medical community regarding the benefits and harms of supplemental screening strategies. An additional concern is the subjective nature of breast density assessment, which is based on the Breast Imaging Reporting and Data System (BI-RADS) that provides four possible categories for breast density.
05 Jul Risk of Staph Bacteremia Can Run in Families
MedicalResearch.com Interview with: Louise Bruun Østergaard MD. Ph.D student Faculty of Medicine and Faculty of Engineering and Science Aalborg University Department of Cardiology, Gentofte Hospital Hellerup MedicalResearch.com: What is the background for this study? What are the main findings? Response: Staphylococcus aureus bacteremia strikes people of all ages resulting in devastating consequence even in young and healthy individuals. Animal studies have shown that the susceptibility to Staphylococcus aureus differs among different genetic strains in mice, suggesting that genetic differences could influence the susceptibility to Staphylococcus aureus in other spices. As a first step in determining whether genetics influence risk of Staphylococcus aureus infections we aimed to study whether a family history of Staphylococcus aureus bacteremia in first-degree relatives was associated with risk of the disease.28 Jun Prehypertension in Pregnancy Linked to Postpartum Metabolic Syndrome
Posted at 16:07h
in Annals Internal Medicine, Author Interviews, Blood Pressure - Hypertension, Metabolic Syndrome, OBGYNE
MedicalResearch.com Interview with:
[caption id="attachment_25658" align="alignleft" width="153"] Dr. Jian Min Niu[/caption]
Dr. Jian-Min Niu
Department of Obstetrics
Guangdong Women and Children Hospita
Guangzhou , China
MedicalResearch.com: What is the background for this study?
Response: Physiological alteration leads to the question of whether the criteria for the diagnosis of gestational hypertension are suitable because the current criteria (systolic BP [SBP] ≥140 mm Hg and diastolic BP [DBP] ≥90 mm Hg) are derived from the non-pregnant population. The optimal blood pressure levels in pregnant women remain an open question. Recent studies have demonstrated associations between prehypertension before pregnancy and hypertensive disorders during pregnancy and gestational diabetes mellitus. To our knowledge, the association between prehypertension during pregnancy and postpartum cardiovascular risk has not been addressed.
Dr. Jian Min Niu[/caption]
Dr. Jian-Min Niu
Department of Obstetrics
Guangdong Women and Children Hospita
Guangzhou , China
MedicalResearch.com: What is the background for this study?
Response: Physiological alteration leads to the question of whether the criteria for the diagnosis of gestational hypertension are suitable because the current criteria (systolic BP [SBP] ≥140 mm Hg and diastolic BP [DBP] ≥90 mm Hg) are derived from the non-pregnant population. The optimal blood pressure levels in pregnant women remain an open question. Recent studies have demonstrated associations between prehypertension before pregnancy and hypertensive disorders during pregnancy and gestational diabetes mellitus. To our knowledge, the association between prehypertension during pregnancy and postpartum cardiovascular risk has not been addressed.
28 Jun Prescribing Naloxone To Patients on Chronic Opioids Reduces ER Visits for Opioid Concerns
MedicalResearch.com Interview with: [caption id="attachment_25429" align="alignleft" width="170"] Dr. Phillip Coffin[/caption]
Phillip O. Coffin, MD, MIA
Director of Substance Use Research
San Francisco Department of Public Health
Assistant Professor, Division of HIV, ID & Global Health
University of California, San Francisco
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: San Francisco has a longstanding naloxone distribution program that primarily works out of syringe exchange programs and is temporally associated with a substantial decline in opioid overdose death due to heroin or involving injection drug use. Over 90% of opioid overdose deaths from 2010-2012 were due to prescription opioids in the absence of heroin, and most of those decedents were prescribed opioids in primary care settings. Based on these data, as well as anecdotal reports from sites such as U.S. Army Fort Bragg in North Carolina - where providing naloxone to pain patients appeared to be associated with a radical decline in opioid overdose admissions to the emergency department - we implemented a naloxone prescribing program in the safety net primary care clinics.
We recommended that providers offer naloxone to all patients who used opioids on a regular basis, or were otherwise at risk for experiencing or witnessing an opioid overdose, although we only measured outcomes related to patients who were prescribed opioids for chronic pain. We also recommended that providers avoid the term "overdose" as that term does not properly reflect the epidemiology of opioid poisoning and is interpreted by many to mean intentionally consuming a large amount of opioids; instead we recommended saying things like: "Opioids can cause bad reactions where you stop breathing or can't be woken up." Providers prescribed mostly the jerry-rigged nasal device, with the atomizer and a brochure dispensed at clinic and the naloxone picked up at the patients' usual pharmacies, to approximate real-world medical practice.
Dr. Phillip Coffin[/caption]
Phillip O. Coffin, MD, MIA
Director of Substance Use Research
San Francisco Department of Public Health
Assistant Professor, Division of HIV, ID & Global Health
University of California, San Francisco
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: San Francisco has a longstanding naloxone distribution program that primarily works out of syringe exchange programs and is temporally associated with a substantial decline in opioid overdose death due to heroin or involving injection drug use. Over 90% of opioid overdose deaths from 2010-2012 were due to prescription opioids in the absence of heroin, and most of those decedents were prescribed opioids in primary care settings. Based on these data, as well as anecdotal reports from sites such as U.S. Army Fort Bragg in North Carolina - where providing naloxone to pain patients appeared to be associated with a radical decline in opioid overdose admissions to the emergency department - we implemented a naloxone prescribing program in the safety net primary care clinics.
We recommended that providers offer naloxone to all patients who used opioids on a regular basis, or were otherwise at risk for experiencing or witnessing an opioid overdose, although we only measured outcomes related to patients who were prescribed opioids for chronic pain. We also recommended that providers avoid the term "overdose" as that term does not properly reflect the epidemiology of opioid poisoning and is interpreted by many to mean intentionally consuming a large amount of opioids; instead we recommended saying things like: "Opioids can cause bad reactions where you stop breathing or can't be woken up." Providers prescribed mostly the jerry-rigged nasal device, with the atomizer and a brochure dispensed at clinic and the naloxone picked up at the patients' usual pharmacies, to approximate real-world medical practice.
22 Jun Pioglitazone Is Safe and Effective Option For Patients with Type 2 Diabetes and NASH
Posted at 18:17h
in Annals Internal Medicine, Author Interviews, Diabetes, Hepatitis - Liver Disease, Pharmacology
MedicalResearch.com Interview with:
[caption id="attachment_25367" align="alignleft" width="168"] Dr. Kenneth Cusi[/caption]
Kenneth Cusi, M.D., F.A.C.P., F.A.C.E.
Professor of Medicine
VAMC staff
Chief, Division of Endocrinology, Diabetes and Metabolism
The University of Florida
Gainesville, FL 32610-0226
MedicalResearch.com: What is the background for this study?
Dr. Cusi: Many patients with prediabetes or Type 2 Diabetes Mellitus (T2DM) are not diagnosed with Nonalcoholic steatohepatitis (NASH), a disease that is the second cause of liver transplantation in the United States. It is also associated with worse cardiovascular disease and harder to control T2DM. We had done in this population a proof-of-concept study published in Nov 2006 in the NEJM. But we lacked a larger, long-term study for definitive proof. This is the largest SINGLE center study, and the longest ever (3 years).
NASH is an overlooked problem for perhaps as many as one-third of patients with Type 2 Diabetes Mellitus. There is now a safe and effective treatment option for patients with T2DM and NASH – pioglitazone will become for NASH what metformin is to the treatment of T2DM: a safe, effective, the “backbone therapy" to which other treatments will be added.
Dr. Kenneth Cusi[/caption]
Kenneth Cusi, M.D., F.A.C.P., F.A.C.E.
Professor of Medicine
VAMC staff
Chief, Division of Endocrinology, Diabetes and Metabolism
The University of Florida
Gainesville, FL 32610-0226
MedicalResearch.com: What is the background for this study?
Dr. Cusi: Many patients with prediabetes or Type 2 Diabetes Mellitus (T2DM) are not diagnosed with Nonalcoholic steatohepatitis (NASH), a disease that is the second cause of liver transplantation in the United States. It is also associated with worse cardiovascular disease and harder to control T2DM. We had done in this population a proof-of-concept study published in Nov 2006 in the NEJM. But we lacked a larger, long-term study for definitive proof. This is the largest SINGLE center study, and the longest ever (3 years).
NASH is an overlooked problem for perhaps as many as one-third of patients with Type 2 Diabetes Mellitus. There is now a safe and effective treatment option for patients with T2DM and NASH – pioglitazone will become for NASH what metformin is to the treatment of T2DM: a safe, effective, the “backbone therapy" to which other treatments will be added.
21 Jun Physician Extenders Utilize Similar Rates of Low Value Services as Primary Care Physicians
MedicalResearch.com Interview with: [caption id="attachment_25285" align="alignleft" width="130"] Dr. John Mafi[/caption]
John N. Mafi, MD, MPH
Assistant Professor of Medicine
Division of General Internal Medicine and Health Services Research
UCLA David Geffen School of Medicine
Los Angeles, CA 90024
Affiliated Adjunct in Health Policy
RAND Corporation
Santa Monica, CA 90401
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Mafi: The U.S. healthcare system faces a looming shortage of primary care physicians, with some estimates as high as 20,000 physicians by the year 2020. In addition, fewer and fewer trainees enter primary care careers because of the harder work and lower salaries. Combine this with the passage of the Affordable Care Act and the millions of newly insured patients looking for a primary care provider, and you have created a perfect storm where timely access to primary care becomes essentially unachievable.
Many advocate for expanding the role of nurse practitioners and physician assistants to mitigate the physician shortage. But this is controversial as most doctors believe nurse practitioners provide inferior care to doctors and many feel that expanding their role would worsen the value and efficiency of the U.S. healthcare system.
While studies suggest they provide similar quality of care to physicians, few have actually evaluated whether they provide greater amounts of inefficient or low value care. Low value care is important because it can harm patients (antibiotics for colds don’t help patients and have harmful side effects) and they can raise healthcare costs. In this context, we used a large national database on ambulatory visits to compare the quality and efficiency of care among nurse practitioners, physician assistants, and physicians in the U.S. primary care setting.
In our 15 year analysis of nearly 29,000 patients who saw either a nurse practitioner, physician assistant, or a physician, we found similar rates of inappropriate antibiotic use for colds, unnecessary imaging (such as x-rays, CT scans, and MRI scans) for back pain and headache, and potentially necessary referrals to specialists for these same three conditions.
Dr. John Mafi[/caption]
John N. Mafi, MD, MPH
Assistant Professor of Medicine
Division of General Internal Medicine and Health Services Research
UCLA David Geffen School of Medicine
Los Angeles, CA 90024
Affiliated Adjunct in Health Policy
RAND Corporation
Santa Monica, CA 90401
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Mafi: The U.S. healthcare system faces a looming shortage of primary care physicians, with some estimates as high as 20,000 physicians by the year 2020. In addition, fewer and fewer trainees enter primary care careers because of the harder work and lower salaries. Combine this with the passage of the Affordable Care Act and the millions of newly insured patients looking for a primary care provider, and you have created a perfect storm where timely access to primary care becomes essentially unachievable.
Many advocate for expanding the role of nurse practitioners and physician assistants to mitigate the physician shortage. But this is controversial as most doctors believe nurse practitioners provide inferior care to doctors and many feel that expanding their role would worsen the value and efficiency of the U.S. healthcare system.
While studies suggest they provide similar quality of care to physicians, few have actually evaluated whether they provide greater amounts of inefficient or low value care. Low value care is important because it can harm patients (antibiotics for colds don’t help patients and have harmful side effects) and they can raise healthcare costs. In this context, we used a large national database on ambulatory visits to compare the quality and efficiency of care among nurse practitioners, physician assistants, and physicians in the U.S. primary care setting.
In our 15 year analysis of nearly 29,000 patients who saw either a nurse practitioner, physician assistant, or a physician, we found similar rates of inappropriate antibiotic use for colds, unnecessary imaging (such as x-rays, CT scans, and MRI scans) for back pain and headache, and potentially necessary referrals to specialists for these same three conditions.
20 Jun Single-Step Testing Can Improve Access To Hepatitis C Testing
Posted at 22:44h
in Annals Internal Medicine, Author Interviews, Cost of Health Care, Hepatitis - Liver Disease
MedicalResearch.com Interview with:
[caption id="attachment_25322" align="alignleft" width="160"] Dr. Morgan Freiman[/caption]
J. Morgan Freiman, MD
Infectious disease research fellow
Boston Medical Center
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Freiman: There are 130-150 million persons infected with chronic HCV with 75% of all cases occurring in low- and middle- income countries (LMICs). Diagnosis is a 2-step process that starts with screening for exposure with an assay that detects antibodies to HCV (anti-HCV), followed by nucleic acid testing (NAT) for persons with reactive anti-HCV to measure HCV ribonucleic acid (RNA) and confirm active viremia.
In LMICs diagnostic capacity is low, and fewer than 1% of patients are aware of their infection. Additionally, a significant proportion of patients who test positive for anti-HCV are lost to follow-up before nucleic acid testing. The 2-step diagnostic process is thus a major bottleneck to the HCV cascade of care. Testing for hepatitis C virus core antigen (HCVcAg) is a potential replacement for NAT.
Our systematic review evaluated the accuracy of diagnosis of active HCV infection among adults and children for 5 commercially available HCVcAg tests compared with NAT. We found that HCVcAg assays with signal amplification have high sensitivity, high specificity, and have the potential to replace NAT in settings with high HCV prevalence.
Dr. Morgan Freiman[/caption]
J. Morgan Freiman, MD
Infectious disease research fellow
Boston Medical Center
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Freiman: There are 130-150 million persons infected with chronic HCV with 75% of all cases occurring in low- and middle- income countries (LMICs). Diagnosis is a 2-step process that starts with screening for exposure with an assay that detects antibodies to HCV (anti-HCV), followed by nucleic acid testing (NAT) for persons with reactive anti-HCV to measure HCV ribonucleic acid (RNA) and confirm active viremia.
In LMICs diagnostic capacity is low, and fewer than 1% of patients are aware of their infection. Additionally, a significant proportion of patients who test positive for anti-HCV are lost to follow-up before nucleic acid testing. The 2-step diagnostic process is thus a major bottleneck to the HCV cascade of care. Testing for hepatitis C virus core antigen (HCVcAg) is a potential replacement for NAT.
Our systematic review evaluated the accuracy of diagnosis of active HCV infection among adults and children for 5 commercially available HCVcAg tests compared with NAT. We found that HCVcAg assays with signal amplification have high sensitivity, high specificity, and have the potential to replace NAT in settings with high HCV prevalence.
17 Jun ClinicalTrials.gov and Drugs@fda.gov Report Complementary Information
MedicalResearch.com Interview with: [caption id="attachment_25281" align="alignleft" width="180"] Dr. Steven Woloshin[/caption]
Steven Woloshin, MD
Professor of The Dartmouth Institute
Professor of Medicine
Professor of Community and Family Medicine
New Hamphsire
MedicalResearch.com: What is the background for this study?
Dr. Woloshin: Drug companies are required by law to post results of trials used to support drug applications to the FDA on the clinicaltrials.gov website - but it is not clear whether posted results are complete and accurate. Recent studies attempting to validate posted results by comparing them to corresponding peer reviewed medical journal publications suggest that discrepancies are relatively common. But it is which source is more likely to be correct. We tried to validate posted results against an arguably better gold standard, the drug approval packages from the FDA (ie, the medical and statistical reviews posted on the drugs@fda.gov website). FDA reviews have an advantage over peer reviewed publications: unlike medical journal editors and peer reviewers, FDA has access to the individual participant data from the trials. This means FDA can see all the trials and all the outcomes (avoiding sleective publication) and it means FDA can independently reanalyze according to what they believe to be the best statistical practices (data can be analyzed in many ways - and different decisions, for example, how to account for missing data, can yield very different results).
Dr. Steven Woloshin[/caption]
Steven Woloshin, MD
Professor of The Dartmouth Institute
Professor of Medicine
Professor of Community and Family Medicine
New Hamphsire
MedicalResearch.com: What is the background for this study?
Dr. Woloshin: Drug companies are required by law to post results of trials used to support drug applications to the FDA on the clinicaltrials.gov website - but it is not clear whether posted results are complete and accurate. Recent studies attempting to validate posted results by comparing them to corresponding peer reviewed medical journal publications suggest that discrepancies are relatively common. But it is which source is more likely to be correct. We tried to validate posted results against an arguably better gold standard, the drug approval packages from the FDA (ie, the medical and statistical reviews posted on the drugs@fda.gov website). FDA reviews have an advantage over peer reviewed publications: unlike medical journal editors and peer reviewers, FDA has access to the individual participant data from the trials. This means FDA can see all the trials and all the outcomes (avoiding sleective publication) and it means FDA can independently reanalyze according to what they believe to be the best statistical practices (data can be analyzed in many ways - and different decisions, for example, how to account for missing data, can yield very different results).
15 Jun Cardiovascular Risks More Common With Newer TKI Chemotherapeutics for CML
Posted at 15:54h
in Annals Internal Medicine, Author Interviews, Chemotherapy, Heart Disease, Karolinski Institute, Leukemia
MedicalResearch.com Interview with:
Torsten Dahlén MD
Centre for Hematology
Karolinska University Hospital Solna
Stockholm Sweden
MedicalResearch.com: What is the background for this study?
Dr. Dahlén: Patients diagnosed with CML have had a dramatic increase in life-expectancy since the widespread introduction of tyrosine kinase inhibitors (TKI) in 2001. However, treatment is today regarded as life-long. We thus need to observe for late-effects of continuous TKI exposure. Recent reports have demonstrated a linkage between TKI treatment, especially more potent 2nd and 3rd generation drugs, and to the occurrence of peripheral arterial occlusive disease (PAOD). This study aimed to use real-world data utilizing Swedish population based registries together with the dedicated Swedish CML registry which contains data and follow-up on more than 98% of all CML patients diagnosed in Sweden since 2002.
07 Jun Suicide Rates Much Higher In Army Than Other Service Lines
MedicalResearch.com Interview with: [caption id="attachment_24973" align="alignleft" width="160"] Dr. Andrew Anglemyer[/caption]
Andrew Anglemyer, PhD MPH
Operations Research Department
U.S. Naval Postgraduate School
Monterey, CA 93943
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Anglemyer: Suicide prevention programs in the military are ubiquitous. We aimed to identify the trends in suicide for each service specifically and explore any nonclinical factors that may be associated with the chosen methods of suicide. The trends in suicide are similar to what others have found.
The differences in those rates between services are striking, though. Not only are most suicides in the active duty military among the Army personnel, but the suicide rate among Army personnel is the highest and has been every year since 2006. Additionally, among Army personnel and Marines who committed suicide, those with an infantry or special operations job classification were significantly more likely to use a firearm to commit suicide than those without those job classifications.
Dr. Andrew Anglemyer[/caption]
Andrew Anglemyer, PhD MPH
Operations Research Department
U.S. Naval Postgraduate School
Monterey, CA 93943
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Anglemyer: Suicide prevention programs in the military are ubiquitous. We aimed to identify the trends in suicide for each service specifically and explore any nonclinical factors that may be associated with the chosen methods of suicide. The trends in suicide are similar to what others have found.
The differences in those rates between services are striking, though. Not only are most suicides in the active duty military among the Army personnel, but the suicide rate among Army personnel is the highest and has been every year since 2006. Additionally, among Army personnel and Marines who committed suicide, those with an infantry or special operations job classification were significantly more likely to use a firearm to commit suicide than those without those job classifications.
04 Apr Nurses Financial Relationships With Industry May Not Be Transparent
[caption id="attachment_23142" align="alignleft" width="200"] Dr. Quinn Grundy[/caption]
MedicalResearch.com Interview with:
Quinn Grundy, PhD, RN
Postdoctoral Research Associate
Charles Perkins Centre
Faculty of Pharmacy
The University of Sydney
MedicalResearch.com: What is the background for this study?
Dr. Grundy: In 2010, United States (US) lawmakers passed the Physician Payments Sunshine Act as part of the Affordable Care Act. The goal of this legislation was to make publicly transparent the financial relationships between physicians and pharmaceutical and medical device companies. These relationships are associated with increased prescribing of high cost, brand name medications with limited track records for safety. Policymakers hoped that increased transparency would help to deter relationships between physicians and industry that could bias treatment decision-making in this way.
What caught our attention was that nurses, though they represent the largest proportion of health professionals, are omitted from the US Sunshine legislation. We questioned whether policymakers believed that nurses did not have the same kinds of relationships with industry as their physician counterparts, or, whether they did not believe that the consequences of nurse-industry interactions would warrant regulation.
Rather than assuming that nurses interacted with industry in the same way that physicians do, we conducted an exploratory, in-depth qualitative study of nurses’ interactions with industry representatives in day-to-day clinical practice. At 4 hospitals in the western US, we interviewed 72 nurses, hospital administrators, supply chain professionals and industry representatives. Over a period of 2 years, we also directly observed nurses’ interactions with what we call “medically-related” industry, including pharmaceutical, medical equipment and device, infant formula, and health technology companies.
Dr. Quinn Grundy[/caption]
MedicalResearch.com Interview with:
Quinn Grundy, PhD, RN
Postdoctoral Research Associate
Charles Perkins Centre
Faculty of Pharmacy
The University of Sydney
MedicalResearch.com: What is the background for this study?
Dr. Grundy: In 2010, United States (US) lawmakers passed the Physician Payments Sunshine Act as part of the Affordable Care Act. The goal of this legislation was to make publicly transparent the financial relationships between physicians and pharmaceutical and medical device companies. These relationships are associated with increased prescribing of high cost, brand name medications with limited track records for safety. Policymakers hoped that increased transparency would help to deter relationships between physicians and industry that could bias treatment decision-making in this way.
What caught our attention was that nurses, though they represent the largest proportion of health professionals, are omitted from the US Sunshine legislation. We questioned whether policymakers believed that nurses did not have the same kinds of relationships with industry as their physician counterparts, or, whether they did not believe that the consequences of nurse-industry interactions would warrant regulation.
Rather than assuming that nurses interacted with industry in the same way that physicians do, we conducted an exploratory, in-depth qualitative study of nurses’ interactions with industry representatives in day-to-day clinical practice. At 4 hospitals in the western US, we interviewed 72 nurses, hospital administrators, supply chain professionals and industry representatives. Over a period of 2 years, we also directly observed nurses’ interactions with what we call “medically-related” industry, including pharmaceutical, medical equipment and device, infant formula, and health technology companies.
27 Mar PCSK9 Antibody May Revolutionize Treatment of Atherosclerosis and Acute Coronary Syndrome
Posted at 15:42h
in Annals Internal Medicine, Author Interviews, Duke, Heart Disease, Johns Hopkins, Lipids
MedicalResearch.com Interview with: [caption id="attachment_22792" align="alignleft" width="186"] Dr. Paul Gurbel[/caption] Paul A. Gurbel, M.D. Director, Inova Center for Thrombosis Research and Drug Development Director, Cardiovascular Medicine Research Director, Interventional Cardiology Inova Heart and Vascular Institute Falls Church, VA Professor of Medicine, Johns Hopkins University School of Medicine Adjunct Professor of Medicine, Duke University School of Medicine MedicalResearch.com: What is the background for...
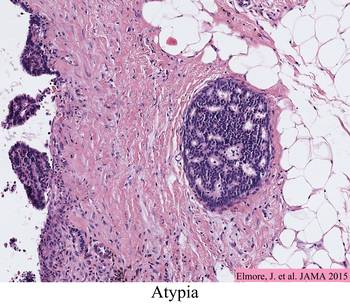
21 Mar Pathologists Often Disagree On Atypia or DCIS in Breast Biopsies
MedicalResearch.com Interview with: [caption id="attachment_22799" align="alignleft" width="161"] Dr. Joann Elmore[/caption]
Joann G. Elmore M.D., M.P.H.
Professor of Medicine,
Adjunct Professor of Epidemiology,
University of Washington School of Medicine
Harborview Medical Center
Seattle, WA 98104-2499
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Elmore: Our team began studying diagnostic agreement among pathologists while interpreting breast biopsies in 2009. Early findings from the Breast Pathology Study (B-Path) were published in March 2015 in the Journal of the American Medical Association and indicated strong agreement among pathologists when diagnosing invasive breast cancer or benign breast tissue. Agreement, however, was much lower for ductal carcinoma in situ (DCIS) and atypia. Results from this study raised concerns that a high percentage of breast biopsies may be inaccurately diagnosed. These concerns were amplified in the media with statements like “as many as one-in-four biopsies are incorrectly diagnosed.” Statements like this inaccurately depicted the results of our study, which included a test set weighted heavily with DCIS and atypia cases. It is important to consider the percentage that each outcome category contributes to the overall number of biopsies in the U.S. population as we found that the agreement rate of pathologists varies drastically across these diagnostic categories.
Dr. Joann Elmore[/caption]
Joann G. Elmore M.D., M.P.H.
Professor of Medicine,
Adjunct Professor of Epidemiology,
University of Washington School of Medicine
Harborview Medical Center
Seattle, WA 98104-2499
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Elmore: Our team began studying diagnostic agreement among pathologists while interpreting breast biopsies in 2009. Early findings from the Breast Pathology Study (B-Path) were published in March 2015 in the Journal of the American Medical Association and indicated strong agreement among pathologists when diagnosing invasive breast cancer or benign breast tissue. Agreement, however, was much lower for ductal carcinoma in situ (DCIS) and atypia. Results from this study raised concerns that a high percentage of breast biopsies may be inaccurately diagnosed. These concerns were amplified in the media with statements like “as many as one-in-four biopsies are incorrectly diagnosed.” Statements like this inaccurately depicted the results of our study, which included a test set weighted heavily with DCIS and atypia cases. It is important to consider the percentage that each outcome category contributes to the overall number of biopsies in the U.S. population as we found that the agreement rate of pathologists varies drastically across these diagnostic categories.
 In the new work published in Annals of Internal Medicine, we have analyzed the B-Path results to reflect variation among diagnoses of women using U.S. population-adjusted estimates,
In an effort to help physicians and patients better understand what the B-Path results mean for women, we have analyzed the B-Path results to reflect variation among diagnoses of women using U.S. population-adjusted estimates. When adjusted using population-based predictive value estimates, the B-Path results indicate that pathologists’ overall interpretations of breast biopsies would be confirmed by an expert panel 92 out of 100 biopsies, with more of the initial diagnoses over-interpreted rather than under-interpreted.
Of concern, our results noted that among 100 breast biopsies given an initial diagnosis of atypia, less than half of these cases would be given a diagnosis of atypia after review by a panel of three experienced breast pathologists. Over half of the biopsies would be downgraded from atypia to a diagnosis of benign without atypia after review.
In the new work published in Annals of Internal Medicine, we have analyzed the B-Path results to reflect variation among diagnoses of women using U.S. population-adjusted estimates,
In an effort to help physicians and patients better understand what the B-Path results mean for women, we have analyzed the B-Path results to reflect variation among diagnoses of women using U.S. population-adjusted estimates. When adjusted using population-based predictive value estimates, the B-Path results indicate that pathologists’ overall interpretations of breast biopsies would be confirmed by an expert panel 92 out of 100 biopsies, with more of the initial diagnoses over-interpreted rather than under-interpreted.
Of concern, our results noted that among 100 breast biopsies given an initial diagnosis of atypia, less than half of these cases would be given a diagnosis of atypia after review by a panel of three experienced breast pathologists. Over half of the biopsies would be downgraded from atypia to a diagnosis of benign without atypia after review.
16 Mar Hospital Stays Provide Opportunity to Vaccinate High Risk Patients
Posted at 13:48h
in Annals Internal Medicine, Author Interviews, Flu - Influenza, Kaiser Permanente, Surgical Research, Vaccine Studies
MedicalResearch.com Interview with:
[caption id="attachment_22564" align="alignleft" width="142"] Dr. Sarah Tartoff[/caption]
Sara Y. Tartof, PhD, MPH
Kaiser Permanente Southern California Department of Research & Evaluation
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Tartof: The flu is a highly contagious respiratory infection that can cause serious complications, hospitalizations and, in some cases, even death. Some people, such as older adults, young children and people with certain health conditions, are at high risk for serious complications. In addition to recommending annual flu vaccination for people 6 months of age and older, the Centers for Disease Control and Prevention recommends that hospitalized patients who are eligible receive the flu vaccine before discharge.
Historically, inpatient rates of vaccination have been low. There has been concern among surgeons that vaccinating patients while they are in the hospital can contribute to increased risk of vaccine-related fever or muscle pain, which might be incorrectly attributed to surgical complications. However, there have been no data to support that concern. The objective of this study was to provide clinical evidence that would either substantiate or refute concerns about the safety of perioperative vaccination.
Dr. Sarah Tartoff[/caption]
Sara Y. Tartof, PhD, MPH
Kaiser Permanente Southern California Department of Research & Evaluation
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Tartof: The flu is a highly contagious respiratory infection that can cause serious complications, hospitalizations and, in some cases, even death. Some people, such as older adults, young children and people with certain health conditions, are at high risk for serious complications. In addition to recommending annual flu vaccination for people 6 months of age and older, the Centers for Disease Control and Prevention recommends that hospitalized patients who are eligible receive the flu vaccine before discharge.
Historically, inpatient rates of vaccination have been low. There has been concern among surgeons that vaccinating patients while they are in the hospital can contribute to increased risk of vaccine-related fever or muscle pain, which might be incorrectly attributed to surgical complications. However, there have been no data to support that concern. The objective of this study was to provide clinical evidence that would either substantiate or refute concerns about the safety of perioperative vaccination.
15 Mar Quitting Smoking Cold Turkey Leads To More Success
MedicalResearch.com Interview with: [caption id="attachment_22551" align="alignleft" width="200"] Dr. Lindson-Hawley[/caption]
Dr Nicola Lindson-Hawley PhD
Cochrane Tobacco Addiction Group (TAG) Managing Editor
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Lindson-Hawley: For many people, the obvious way to quit smoking is to cut down gradually until they stop. After all, that’s how we accomplish most other goals that are hard. With addictions other than smoking, we aim to get people to cut down gradually rather than stop abruptly. But with smoking, the norm is to advise people to stop all at once. Around the world, physicians and others who support smoking cessation help people to quit abruptly and not to cut down first. However, if physicians are not providing support to people who want to quit by reduction, then they will have less chance of success as we know that people who receive support to quit are more likely to succeed. On the other hand, if cutting down is a bad way to quit, then we need to persuade people to abandon their common sense idea and quit abruptly instead. Therefore, this study investigated this by comparing a group of smokers advised to quit gradually by cutting down with a group who quit all at once. What we found was that cutting down first, was a less successful way to quit than smoking as normal and then stopping. Smokers who quit abruptly were 25% more likely to have quit after 4 weeks than those who quit gradually.
Dr. Lindson-Hawley[/caption]
Dr Nicola Lindson-Hawley PhD
Cochrane Tobacco Addiction Group (TAG) Managing Editor
MedicalResearch.com: What is the background for this study? What are the main findings?
Dr. Lindson-Hawley: For many people, the obvious way to quit smoking is to cut down gradually until they stop. After all, that’s how we accomplish most other goals that are hard. With addictions other than smoking, we aim to get people to cut down gradually rather than stop abruptly. But with smoking, the norm is to advise people to stop all at once. Around the world, physicians and others who support smoking cessation help people to quit abruptly and not to cut down first. However, if physicians are not providing support to people who want to quit by reduction, then they will have less chance of success as we know that people who receive support to quit are more likely to succeed. On the other hand, if cutting down is a bad way to quit, then we need to persuade people to abandon their common sense idea and quit abruptly instead. Therefore, this study investigated this by comparing a group of smokers advised to quit gradually by cutting down with a group who quit all at once. What we found was that cutting down first, was a less successful way to quit than smoking as normal and then stopping. Smokers who quit abruptly were 25% more likely to have quit after 4 weeks than those who quit gradually.