MedicalResearch.com Interview with:
[caption id="attachment_57406" align="alignleft" width="200"]

Dr. Hoberman[/caption]
Alejandro Hoberman, M.D.
Vice Chair of Clinical Research, Division Director, General Academic Pediatrics, and Professor of Pediatrics and Clinical and Translational Science
Jack L. Paradise, MD Endowed Professor of Pediatric Research, UPMC Children's Hospital of PittsburghPresident, UPMC Children's Community Pediatrics
MedicalResearch.com: What is the background for this study?
Response: Acute otitis media (AOM) is the most frequently diagnosed illness in children in the United States for which antibiotics are prescribed. Recurrent AOM is the principal indication for tympanostomy-tube placement, the most frequently performed operation in children after the newborn period. Supporting the performance of tympanostomy-tube placement for recurrent acute otitis media has been the commonplace observation, after surgery, of acute otitis media–free periods of varying duration. Counterbalancing this view have been the cost of tympanostomy-tube placement; risks and possible late sequelae of anesthesia in young children; the possible occurrence of refractory tube otorrhea, tube blockage, premature extrusion, or dislocation of the tube into the middle-ear cavity; various structural tympanic membrane sequelae; and the possible development of mild conductive hearing loss. Tempering support for surgery is the progressive reduction in the incidence of acute otitis media that usually accompanies a child’s increasing age.
Previous trials of tympanostomy-tube placement for recurrent acute otitis media, all conducted before the introduction of pneumococcal conjugate vaccine, have given mixed results and were limited, variously, by small sample size, uncertain validity of diagnoses of acute otitis media determining trial eligibility, short periods of follow-up, and substantial attrition of participants. Official recommendations regarding tympanostomy-tube placement for children with recurrent acute otitis media differ — an otolaryngologic guideline recommends the procedure for children with recurrent acute otitis media, provided that middle-ear effusion is present in at least one ear; a contemporaneous pediatric guideline discusses tympanostomy-tube placement as an “option [that] clinicians may offer.”
Given these uncertainties, we undertook the present trial involving children 6 to 35 months of age who had a history of recurrent acute otitis media to determine whether tympanostomy-tube placement, as compared with medical management (comprising episodic antimicrobial treatment, with the option of tympanostomy-tube placement in the event of treatment failure), would result in a greater reduction in the children’s rate of recurrence of acute otitis media during the ensuing 2-year period.




 Dr. Mapara[/caption]
Markus Y Mapara, MD
Professor of Medicine
Director of the Blood and Marrow Transplantation
Columbia University Medical Center
MedicalResearch.com: What is the background for this study? What are the main findings?
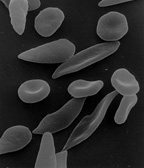
Response: Sickle cell disease is caused by a point mutation in the beta-globin gene of hemoglobin resulting in the production of abnormal hemoglobin which leads to formation of sickle-shaped RBC under conditions of low oxygen. Sickle cell disease affects about 100,000 patients in the US which are predominantly African American. The only curative approach is to perform an allogeneic bone marrow transplant which is however fraught with significant treatment-related risks if a matched sibling donor is not available.
The current study describes the successful application of a novel gene therapy to treat patients with sickle cell disease. The strategy is based on a gene-addition approach to introduce the genetic information for a Hemoglobin F-like molecule termed HgAT87Q into hematopoietic stem cells. The expression of this novel hemoglobin prevents polymerization of HgbS and has now been demonstrated to prevent the occurrence of vaso-occlusive pain crises in sickle cell disease patients.
Dr. Mapara[/caption]
Markus Y Mapara, MD
Professor of Medicine
Director of the Blood and Marrow Transplantation
Columbia University Medical Center
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Sickle cell disease is caused by a point mutation in the beta-globin gene of hemoglobin resulting in the production of abnormal hemoglobin which leads to formation of sickle-shaped RBC under conditions of low oxygen. Sickle cell disease affects about 100,000 patients in the US which are predominantly African American. The only curative approach is to perform an allogeneic bone marrow transplant which is however fraught with significant treatment-related risks if a matched sibling donor is not available.
The current study describes the successful application of a novel gene therapy to treat patients with sickle cell disease. The strategy is based on a gene-addition approach to introduce the genetic information for a Hemoglobin F-like molecule termed HgAT87Q into hematopoietic stem cells. The expression of this novel hemoglobin prevents polymerization of HgbS and has now been demonstrated to prevent the occurrence of vaso-occlusive pain crises in sickle cell disease patients.



 Dr. Dickerman[/caption]
Dr. Barbra Dickerman, PhD
CAUSALab investigator and instructor
Department of Epidemiology
Harvard T.H. Chan School of Public Health
MedicalResearch.com: What is the background for this study?
Response: Early randomized trials showed that the BNT162b2 (Pfizer-BioNTech) and mRNA-1273 (Moderna) vaccines were both remarkably effective at preventing symptomatic disease, when comparing each vaccine with no vaccine. However, head-to-head comparisons of these vaccines have been lacking, leaving open the question of which vaccine is more effective.
In this study, we analyzed the VA’s high-quality databases in a way that emulated the design of the hypothetical trial that would have answered this question. Specifically, we used the findings from the original trials to benchmark our methods and then extended them to provide novel evidence for the comparative effectiveness of these two vaccines in a real-world setting and across diverse subgroups and different time periods.
Dr. Dickerman[/caption]
Dr. Barbra Dickerman, PhD
CAUSALab investigator and instructor
Department of Epidemiology
Harvard T.H. Chan School of Public Health
MedicalResearch.com: What is the background for this study?
Response: Early randomized trials showed that the BNT162b2 (Pfizer-BioNTech) and mRNA-1273 (Moderna) vaccines were both remarkably effective at preventing symptomatic disease, when comparing each vaccine with no vaccine. However, head-to-head comparisons of these vaccines have been lacking, leaving open the question of which vaccine is more effective.
In this study, we analyzed the VA’s high-quality databases in a way that emulated the design of the hypothetical trial that would have answered this question. Specifically, we used the findings from the original trials to benchmark our methods and then extended them to provide novel evidence for the comparative effectiveness of these two vaccines in a real-world setting and across diverse subgroups and different time periods. 


 Dr. Tian[/caption]
MedicalResearch.com Interview with:
Maoyi TIAN PhD
Program Head, Digital Health and Head, Injury & Trauma
Senior Research Fellow
The George Institute
MedicalResearch.com: What is the background for this study?
Response: There is clear evidence from the literature that sodium reduction or potassium supplementation can reduce blood pressure. Reduced blood pressure can also lead to a risk reduction for cardiovascular diseases.
Salt substitute is a reduced sodium added potassium product combined those effects. Previous research of salt substitute focus on the blood pressure outcome. There is no evidence if salt substitute can reduce the risk of cardiovascular diseases or pre-mature death. This study provided a definitive evidence for this unaddressed question.
MedicalResearch.com: What are the main findings?
The main findings of the research were:
Dr. Tian[/caption]
MedicalResearch.com Interview with:
Maoyi TIAN PhD
Program Head, Digital Health and Head, Injury & Trauma
Senior Research Fellow
The George Institute
MedicalResearch.com: What is the background for this study?
Response: There is clear evidence from the literature that sodium reduction or potassium supplementation can reduce blood pressure. Reduced blood pressure can also lead to a risk reduction for cardiovascular diseases.
Salt substitute is a reduced sodium added potassium product combined those effects. Previous research of salt substitute focus on the blood pressure outcome. There is no evidence if salt substitute can reduce the risk of cardiovascular diseases or pre-mature death. This study provided a definitive evidence for this unaddressed question.
MedicalResearch.com: What are the main findings?
The main findings of the research were:






 Prof. Reich[/caption]
Prof. Kristian Reich, MD, PhD
Professor for Translational Research in Inflammatory Skin Diseases
Institute for Health Services Research in Dermatology and Nursing
University Medical Center Hamburg-Eppendorf
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Complete skin clearance is an important treatment goal for patients with psoriasis and is closely associated with treatment satisfaction and improved quality of life. However, it remains an unmet need for many patients.
The interleukin (IL)-17 isoforms IL-17A and IL-17F play central roles in psoriasis pathophysiology and are overexpressed in psoriatic tissues. Existing biologic therapies, such as secukinumab, inhibit IL-17A only. However, increasing evidence indicates that IL-17F contributes independently to the pathobiology of plaque psoriasis, and that blocking both IL-17A and IL-17F may lead to more complete suppression of inflammation and superior clinical outcomes, compared with blocking IL‑17A alone.
Bimekizumab is a humanized monoclonal IgG1 antibody that has been designed to selectively inhibit IL-17F in addition to IL-17A.
Prof. Reich[/caption]
Prof. Kristian Reich, MD, PhD
Professor for Translational Research in Inflammatory Skin Diseases
Institute for Health Services Research in Dermatology and Nursing
University Medical Center Hamburg-Eppendorf
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Complete skin clearance is an important treatment goal for patients with psoriasis and is closely associated with treatment satisfaction and improved quality of life. However, it remains an unmet need for many patients.
The interleukin (IL)-17 isoforms IL-17A and IL-17F play central roles in psoriasis pathophysiology and are overexpressed in psoriatic tissues. Existing biologic therapies, such as secukinumab, inhibit IL-17A only. However, increasing evidence indicates that IL-17F contributes independently to the pathobiology of plaque psoriasis, and that blocking both IL-17A and IL-17F may lead to more complete suppression of inflammation and superior clinical outcomes, compared with blocking IL‑17A alone.
Bimekizumab is a humanized monoclonal IgG1 antibody that has been designed to selectively inhibit IL-17F in addition to IL-17A.



 One example of actinic keratoses on scalp
One example of actinic keratoses on scalp









