
MedicalResearch.com Interview with:
[caption id="attachment_56251" align="alignleft" width="200"] Dr. Magnusson[/caption]
Karin Magnusson PT, PhD
Associate Researcher
Lund University and
Norwegian Institute of Public Health
MedicalResearch.com: What is the background for this study?
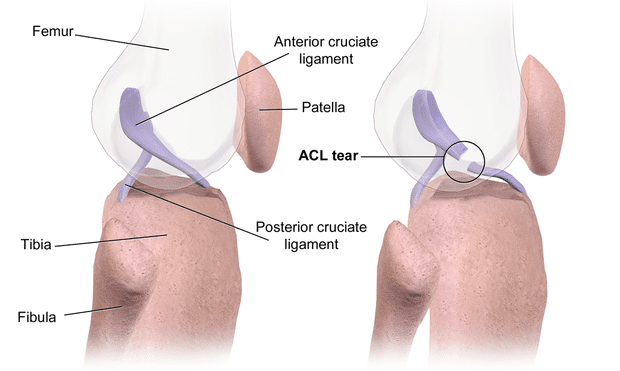
Response: Anterior cruciate ligament (ACL) injury is one of the most common knee injuries, for which very limited data has been presented on the genetic contribution. Based on our knowledge of the role of genetics in the development of ACL-rupture related traits, such as joint hypermobility and knee osteoarthritis, we hypothesized that heritability might play a role also in ACL injury.
Using the Swedish Twin Registry, which is the world's largest twin registry and in this study including more than 88.000 twins, we had unique data to for the first time reliably estimate the heritability for this common knee injury.
Dr. Magnusson[/caption]
Karin Magnusson PT, PhD
Associate Researcher
Lund University and
Norwegian Institute of Public Health
MedicalResearch.com: What is the background for this study?
Response: Anterior cruciate ligament (ACL) injury is one of the most common knee injuries, for which very limited data has been presented on the genetic contribution. Based on our knowledge of the role of genetics in the development of ACL-rupture related traits, such as joint hypermobility and knee osteoarthritis, we hypothesized that heritability might play a role also in ACL injury.
Using the Swedish Twin Registry, which is the world's largest twin registry and in this study including more than 88.000 twins, we had unique data to for the first time reliably estimate the heritability for this common knee injury.
Dr. Magnusson[/caption]
Karin Magnusson PT, PhD
Associate Researcher
Lund University and
Norwegian Institute of Public Health
MedicalResearch.com: What is the background for this study?
Response: Anterior cruciate ligament (ACL) injury is one of the most common knee injuries, for which very limited data has been presented on the genetic contribution. Based on our knowledge of the role of genetics in the development of ACL-rupture related traits, such as joint hypermobility and knee osteoarthritis, we hypothesized that heritability might play a role also in ACL injury.
Using the Swedish Twin Registry, which is the world's largest twin registry and in this study including more than 88.000 twins, we had unique data to for the first time reliably estimate the heritability for this common knee injury. 




 Dr. Chua[/caption]
Isaac Chua, MD, MPH
Division of General Internal Medicine and Primary Care
Brigham and Women's Hospital
MedicalResearch.com: What is the background for this study?
Response: Patient surveys have shown that most people prefer to die at home at the end-of-life. However, during the initial wave of the COVID-19 pandemic, anecdotal evidence from our colleagues and findings from a prior study published in the Journal of the American Geriatrics Society suggested that majority of COVID-19 decedents died in a medical facility. However, less is known about care intensity at the end-of-life according to place of death among patients who died of COVID-19. Therefore, we characterized end-of-life care by place of death among COVID-19 decedents at Mass General Brigham (MGB), the largest health system in Massachusetts.
Dr. Chua[/caption]
Isaac Chua, MD, MPH
Division of General Internal Medicine and Primary Care
Brigham and Women's Hospital
MedicalResearch.com: What is the background for this study?
Response: Patient surveys have shown that most people prefer to die at home at the end-of-life. However, during the initial wave of the COVID-19 pandemic, anecdotal evidence from our colleagues and findings from a prior study published in the Journal of the American Geriatrics Society suggested that majority of COVID-19 decedents died in a medical facility. However, less is known about care intensity at the end-of-life according to place of death among patients who died of COVID-19. Therefore, we characterized end-of-life care by place of death among COVID-19 decedents at Mass General Brigham (MGB), the largest health system in Massachusetts. 
 Dr. Maru[/caption]
Sheela Maru, MD, MPH
Department of Health System Design and Global Health and
Arnhold Institute for Global Health and
Department of Obstetrics, Gynecology and Reproductive Science
Icahn School of Medicine at Mount Sinai
MedicalResearch.com: What is the background for this study?
Response: Universal screening for SARS-CoV-2 infection on Labor and Delivery (L&D) units is a critical strategy to manage patient and health worker safety, especially in a vulnerable high-prevalence community. We describe the results of a SARS-CoV-2 universal screening program at the L&D Unit at Elmhurst Hospital in Queens, NY, a 545-bed public hospital serving a diverse, largely immigrant and low-income patient population and an epicenter of the global pandemic.
Dr. Maru[/caption]
Sheela Maru, MD, MPH
Department of Health System Design and Global Health and
Arnhold Institute for Global Health and
Department of Obstetrics, Gynecology and Reproductive Science
Icahn School of Medicine at Mount Sinai
MedicalResearch.com: What is the background for this study?
Response: Universal screening for SARS-CoV-2 infection on Labor and Delivery (L&D) units is a critical strategy to manage patient and health worker safety, especially in a vulnerable high-prevalence community. We describe the results of a SARS-CoV-2 universal screening program at the L&D Unit at Elmhurst Hospital in Queens, NY, a 545-bed public hospital serving a diverse, largely immigrant and low-income patient population and an epicenter of the global pandemic.


 Dr. Willette[/caption]
Auriel Willette, PhD
Assistant Professor
Food Science and Human Nutrition
Iowa State University
MedicalResearch.com: What is the background for this study?
Response: To date, pharmacology therapies done to slow down or halt Alzheimer's disease have been inconclusive. Lifestyle interventions like changes in diet and activity are also mixed but do show some promise. Dietary clinical trials or self-reported diet have tended to focus on groups of foods such as the Mediterranean or MIND diet. To build from this excellent work, we were curious if we could pinpoint specific foods that were correlated with changes in fluid intelligence over time. Fluid intelligence represents our ability to creatively use existing knowledge, working memory, and other components of "thinking flexibly."
Further, we tested if these patterns of association differed based on genetic risk. In this case, genetic risk was defined as having a family history of Alzheimer's disease or having 1-2 "bad" copies of the Apolipoprotein E (APOE) gene, which is the strongest genetic risk factor for Alzheimer's disease.
Dr. Willette[/caption]
Auriel Willette, PhD
Assistant Professor
Food Science and Human Nutrition
Iowa State University
MedicalResearch.com: What is the background for this study?
Response: To date, pharmacology therapies done to slow down or halt Alzheimer's disease have been inconclusive. Lifestyle interventions like changes in diet and activity are also mixed but do show some promise. Dietary clinical trials or self-reported diet have tended to focus on groups of foods such as the Mediterranean or MIND diet. To build from this excellent work, we were curious if we could pinpoint specific foods that were correlated with changes in fluid intelligence over time. Fluid intelligence represents our ability to creatively use existing knowledge, working memory, and other components of "thinking flexibly."
Further, we tested if these patterns of association differed based on genetic risk. In this case, genetic risk was defined as having a family history of Alzheimer's disease or having 1-2 "bad" copies of the Apolipoprotein E (APOE) gene, which is the strongest genetic risk factor for Alzheimer's disease.

 Dr. McHill[/caption]
Andrew W. McHill, PhD
Research Assistant Professor
Oregon Institute of Occupational Health Sciences
Oregon Health & Science University, Portland OR
Portland, OR 97239
MedicalResearch.com: What is the background for this study?
Response: It has long been known that there is a home court advantage in sports, whether it be due to the home fans cheering, playing within familiar settings, or travel of the opposing team. However, the contribution of travel to home-court advantage could never be fully teased apart due to all the confounds of the other aspects of playing at home.
In March, the National Basketball Association had to pause their season due to COVID-19 concerns, only to start again several months later with the top 22 teams playing in a “bubble” environment where no teams were required to travel. This created a ‘natural experiment’ wherein we could test the impact of travel on winning and performance before the COVID-19 shutdown with games played in the bubble environment with no travel.
Dr. McHill[/caption]
Andrew W. McHill, PhD
Research Assistant Professor
Oregon Institute of Occupational Health Sciences
Oregon Health & Science University, Portland OR
Portland, OR 97239
MedicalResearch.com: What is the background for this study?
Response: It has long been known that there is a home court advantage in sports, whether it be due to the home fans cheering, playing within familiar settings, or travel of the opposing team. However, the contribution of travel to home-court advantage could never be fully teased apart due to all the confounds of the other aspects of playing at home.
In March, the National Basketball Association had to pause their season due to COVID-19 concerns, only to start again several months later with the top 22 teams playing in a “bubble” environment where no teams were required to travel. This created a ‘natural experiment’ wherein we could test the impact of travel on winning and performance before the COVID-19 shutdown with games played in the bubble environment with no travel.

 Asimanshu Das[/caption]
Asimanshu Das, Ph.D. student
Brown University School of Engineering
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Driving in a car with ride-share or car-pool is a widely prevalent social interaction. The study aimed to address the airflows inside cars in various window open/closed configurations using computer simulations, and also looking into the possibility of movement of aerosol-type of particles from one occupant to other.
The main findings are that opening windows provides a likely benefit to reduce the potentially pathogenic aerosols inside the cabin. Generally, more windows the better, but at the least it would be advisable to have one rear side window and one frontside window open.
Asimanshu Das[/caption]
Asimanshu Das, Ph.D. student
Brown University School of Engineering
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Driving in a car with ride-share or car-pool is a widely prevalent social interaction. The study aimed to address the airflows inside cars in various window open/closed configurations using computer simulations, and also looking into the possibility of movement of aerosol-type of particles from one occupant to other.
The main findings are that opening windows provides a likely benefit to reduce the potentially pathogenic aerosols inside the cabin. Generally, more windows the better, but at the least it would be advisable to have one rear side window and one frontside window open.
 Dr. Schmidt[/caption]
William K. Schmidt, Ph.D.
Senior VP Clinical Development
Dr. Schmidt[/caption]
William K. Schmidt, Ph.D.
Senior VP Clinical Development





 Dr. Reed[/caption]
Nicholas S. Reed, AuD
Assistant Professor | Department of Epidemiology
Core Faculty | Cochlear Center for Hearing and Public Health
Johns Hopkins University Bloomberg School of Public Health
MedicalResearch.com: What is the background for this study?
Response: It is known that hearing aid ownership is relatively low in the United States at less than 20% of adults with hearing loss owning and using hearing aids. However, many national estimates of hearing aid ownership are based on data that is over 10 years old. Our team was interested in trying to understand whether ownership in hearing aids had changed over time. We used data from 2011 to 2018 in a nationally representative (United States) observational cohort (The National Health and Aging Trends Study) of Medicare Beneficiaries aged 70 years and older to estimate the change in hearing aid ownership.
In our analysis, the proportion of Medicare beneficiaries 70 years and older who reported owning and using their hearing aids increased 23.3% from 2011 to 2018. However, this growth in ownership was not equal across all older adults. For example, while White males saw a 28.7% increase in hearing aid ownership, Black females saw only a 5.8% increase over the same 8-year period. Moreover, adults living at less than 100% federal poverty level actually saw an overall 13.0% decrease in hearing aid ownership while those living at more than 200% federal poverty line saw an overall 30.6% increase.
Dr. Reed[/caption]
Nicholas S. Reed, AuD
Assistant Professor | Department of Epidemiology
Core Faculty | Cochlear Center for Hearing and Public Health
Johns Hopkins University Bloomberg School of Public Health
MedicalResearch.com: What is the background for this study?
Response: It is known that hearing aid ownership is relatively low in the United States at less than 20% of adults with hearing loss owning and using hearing aids. However, many national estimates of hearing aid ownership are based on data that is over 10 years old. Our team was interested in trying to understand whether ownership in hearing aids had changed over time. We used data from 2011 to 2018 in a nationally representative (United States) observational cohort (The National Health and Aging Trends Study) of Medicare Beneficiaries aged 70 years and older to estimate the change in hearing aid ownership.
In our analysis, the proportion of Medicare beneficiaries 70 years and older who reported owning and using their hearing aids increased 23.3% from 2011 to 2018. However, this growth in ownership was not equal across all older adults. For example, while White males saw a 28.7% increase in hearing aid ownership, Black females saw only a 5.8% increase over the same 8-year period. Moreover, adults living at less than 100% federal poverty level actually saw an overall 13.0% decrease in hearing aid ownership while those living at more than 200% federal poverty line saw an overall 30.6% increase. 


 Prof. Bergee[/caption]
Martin J. Bergee
Professor and Associate Dean for Academic Affairs
School of Music
University of Kansas
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: The idea that listening, participating, or achieving in music makes you better at another subject, say, math, science, or reading, has been around for a while. Indeed, there’s a relationship between achievement in music and achievement in other content areas. But I’ve always assumed that the relationship was spurious, that is, driven my any number of such background influences as urbanicity, ethnicity, SES, level of parent education, the type of school one attends, and so forth. Essentially, I set out to demonstrate once and for all that with these background influences accounted for statistically, the relationship is considerably attenuated. Much to my surprise, however, music achievement’s relationships with reading and math achievement remained quite strong.
Prof. Bergee[/caption]
Martin J. Bergee
Professor and Associate Dean for Academic Affairs
School of Music
University of Kansas
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: The idea that listening, participating, or achieving in music makes you better at another subject, say, math, science, or reading, has been around for a while. Indeed, there’s a relationship between achievement in music and achievement in other content areas. But I’ve always assumed that the relationship was spurious, that is, driven my any number of such background influences as urbanicity, ethnicity, SES, level of parent education, the type of school one attends, and so forth. Essentially, I set out to demonstrate once and for all that with these background influences accounted for statistically, the relationship is considerably attenuated. Much to my surprise, however, music achievement’s relationships with reading and math achievement remained quite strong.

 Sitara Weerakoon[/caption]
Sitara Weerakoon, MPH (she/her)
PhD Candidate | Epidemiology & Biostatistics
Graduate Research Assistant
Center for Pediatric Population Health
UTHealth
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Measures to control the spread of COVID-19 included stay-at-home mandates and business lockdown policies which resulted in many facing a loss of income or employment and more time spent isolated at home. Life stressors (like job loss and social isolation) have been shown to be associated with increased drinking at unhealthy levels. Those with a history of mental health problems may be even more at risk.
We aimed to see if binge drinking (5 or more drinks [male] or 4 or more drinks [female] in one session) and levels of alcohol consumption among binge drinkers were impacted by these pandemic-related factors. We found that increased time spent at home (in weeks) was associated with a 19% increase in the odds of binge drinking and binge drinkers with a previous diagnosis of depression and current depression symptoms (during the early months of the pandemic) had a 237% greater odds of drinking more alcohol (vs drinking the same amount) compared to those with no history and current symptoms of depression.
Sitara Weerakoon[/caption]
Sitara Weerakoon, MPH (she/her)
PhD Candidate | Epidemiology & Biostatistics
Graduate Research Assistant
Center for Pediatric Population Health
UTHealth
MedicalResearch.com: What is the background for this study? What are the main findings?
Response: Measures to control the spread of COVID-19 included stay-at-home mandates and business lockdown policies which resulted in many facing a loss of income or employment and more time spent isolated at home. Life stressors (like job loss and social isolation) have been shown to be associated with increased drinking at unhealthy levels. Those with a history of mental health problems may be even more at risk.
We aimed to see if binge drinking (5 or more drinks [male] or 4 or more drinks [female] in one session) and levels of alcohol consumption among binge drinkers were impacted by these pandemic-related factors. We found that increased time spent at home (in weeks) was associated with a 19% increase in the odds of binge drinking and binge drinkers with a previous diagnosis of depression and current depression symptoms (during the early months of the pandemic) had a 237% greater odds of drinking more alcohol (vs drinking the same amount) compared to those with no history and current symptoms of depression.


 Dr. Jonathan Silverberg[/caption]
Jonathan Silverberg, MD, PHD, MPH
Associate Professor
Director of Clinical Research
Director of Patch Testing
George Washington University School of Medicine and Health Sciences
Washington, DC
MedicalResearch.com: What is the background for this study
Response: Chronic hand eczema was previously shown to be associated with higher rates of allergic contact dermatitis. Yet, little is known about recent trends in North America with respect to the clinical presentation and allergen profile in chronic hand eczema. This study sought to determine the clinical characteristics and etiologies of hand eczema in a large North American cohort of adults referred for patch testing. The patients in the study were patch tested using the North American Contact Dermatitis Group’s allergen screening series.
Dr. Jonathan Silverberg[/caption]
Jonathan Silverberg, MD, PHD, MPH
Associate Professor
Director of Clinical Research
Director of Patch Testing
George Washington University School of Medicine and Health Sciences
Washington, DC
MedicalResearch.com: What is the background for this study
Response: Chronic hand eczema was previously shown to be associated with higher rates of allergic contact dermatitis. Yet, little is known about recent trends in North America with respect to the clinical presentation and allergen profile in chronic hand eczema. This study sought to determine the clinical characteristics and etiologies of hand eczema in a large North American cohort of adults referred for patch testing. The patients in the study were patch tested using the North American Contact Dermatitis Group’s allergen screening series.
 Response: LENVIMA (lenvatinib), discovered and developed by Eisai, is an orally available multiple receptor tyrosine kinase inhibitor that inhibits the kinase activities of vascular endothelial growth factor (VEGF) receptors VEGFR1 (FLT1), VEGFR2 (KDR), and VEGFR3 (FLT4). LENVIMA inhibits other kinases that have been implicated in pathogenic angiogenesis, tumor growth, and cancer progression in addition to their normal cellular functions, including fibroblast growth factor (FGF) receptors FGFR1-4, the platelet derived growth factor receptor alpha (PDGFRα), KIT, and RET.
LENVIMA is approved in combination with everolimus for the treatment of patients with advanced renal cell carcinoma (RCC) following one prior anti-angiogenic therapy. The approved starting dose for LENVIMA is 18 mg daily. The objective of Study 218, a randomized, open-label, Phase 2 trial, was to assess whether the lower starting dose of LENVIMA (14 mg daily) in combination with everolimus (5 mg daily) would provide similar efficacy with an improved safety profile compared to the FDA-approved starting dose of LENVIMA (18 mg daily) plus everolimus (5 mg daily) in patients with advanced renal cell carcinoma (RCC) following prior treatment with an antiangiogenic therapy.
In the US, LENVIMA is also indicated for:
Response: LENVIMA (lenvatinib), discovered and developed by Eisai, is an orally available multiple receptor tyrosine kinase inhibitor that inhibits the kinase activities of vascular endothelial growth factor (VEGF) receptors VEGFR1 (FLT1), VEGFR2 (KDR), and VEGFR3 (FLT4). LENVIMA inhibits other kinases that have been implicated in pathogenic angiogenesis, tumor growth, and cancer progression in addition to their normal cellular functions, including fibroblast growth factor (FGF) receptors FGFR1-4, the platelet derived growth factor receptor alpha (PDGFRα), KIT, and RET.
LENVIMA is approved in combination with everolimus for the treatment of patients with advanced renal cell carcinoma (RCC) following one prior anti-angiogenic therapy. The approved starting dose for LENVIMA is 18 mg daily. The objective of Study 218, a randomized, open-label, Phase 2 trial, was to assess whether the lower starting dose of LENVIMA (14 mg daily) in combination with everolimus (5 mg daily) would provide similar efficacy with an improved safety profile compared to the FDA-approved starting dose of LENVIMA (18 mg daily) plus everolimus (5 mg daily) in patients with advanced renal cell carcinoma (RCC) following prior treatment with an antiangiogenic therapy.
In the US, LENVIMA is also indicated for:

 Dr. Gernand[/caption]
Jeremy M. Gernand
Dr. Gernand[/caption]
Jeremy M. Gernand
 Dr. Soller[/caption]
Lianne Soller, PhD
Allergy Research Manager
BC Children’s Hospital Allergy Clinic
Vancouver, BC, Canada
MedicalResearch.com: What is the background for this study?
Response: Peanut oral immunotherapy (also known as OIT) has been studied for many years in clinical trials and has been found to be safe and effective in preschoolers. However, we know that clinical trials do not always reflect what happens in the real world.
We wanted to see study whether peanut OIT would work as well in the real world. This is a follow up of our preschool peanut OIT safety study published in April 2019 which noted only 0.4% severe reactions and 4% epinephrine use during build-up.
Dr. Soller[/caption]
Lianne Soller, PhD
Allergy Research Manager
BC Children’s Hospital Allergy Clinic
Vancouver, BC, Canada
MedicalResearch.com: What is the background for this study?
Response: Peanut oral immunotherapy (also known as OIT) has been studied for many years in clinical trials and has been found to be safe and effective in preschoolers. However, we know that clinical trials do not always reflect what happens in the real world.
We wanted to see study whether peanut OIT would work as well in the real world. This is a follow up of our preschool peanut OIT safety study published in April 2019 which noted only 0.4% severe reactions and 4% epinephrine use during build-up.


